Antibodies against Eplet mismatches can help identify the cause of ABMR in absence of DSAs on single antigen bead assay in transplantation
Shruti Tapiawala1,2, Suchita Jogale2, Shivani Palshetkar2, Prashant Rajput1, Zaheer Virani1, Hepal Vora1, Bharat Shah1,2.
1Institute of Renal Sciences, Gleneagles Hospital, Mumbai, India; 2Histocompatibility, ATDI Lab Pvt Ltd, Mumbai, India
Introduction: Presence of HLA antibodies against the donor are known to cause antibody mediated rejections and predict an inferior allograft survival. HLA antibodies are recognized against epitopes rather than the whole antigen and eplet mismatches have been proven to increase the risk of De Novo Antibody formation. Presence of Donor specific HLA antibodies (DSA) in the serum assists in diagnosing Antibody mediated rejection (ABMR). Sometimes patients presenting with biopsy proven ABMR may display absence of DSAs but presence of HLA antibodies which are not donor specific. Eplet mismatches common in the HLA antibodies and Donor specific HLA antibodies have been implicated in pathogenesis of ABMR. We report six cases which demonstrate the importance for identifying eplet mismatch load at transplant and identifying antibodies against eplets rather than HLA antigens to diagnose and monitor the allograft.
Methods: Six patients with biopsy proven ABMR and a simultaneous serum sample for single antigen bead (SAB) assay showing presence of HLA antibodies but absence of DSAs were studied. Eplet mismatch load was identified using HLAMatch-maker computer algorithm. Common eplets between the HLA antibodies identified in the patient’s serum and the donor HLA were listed and a virtual crossmatch was performed.
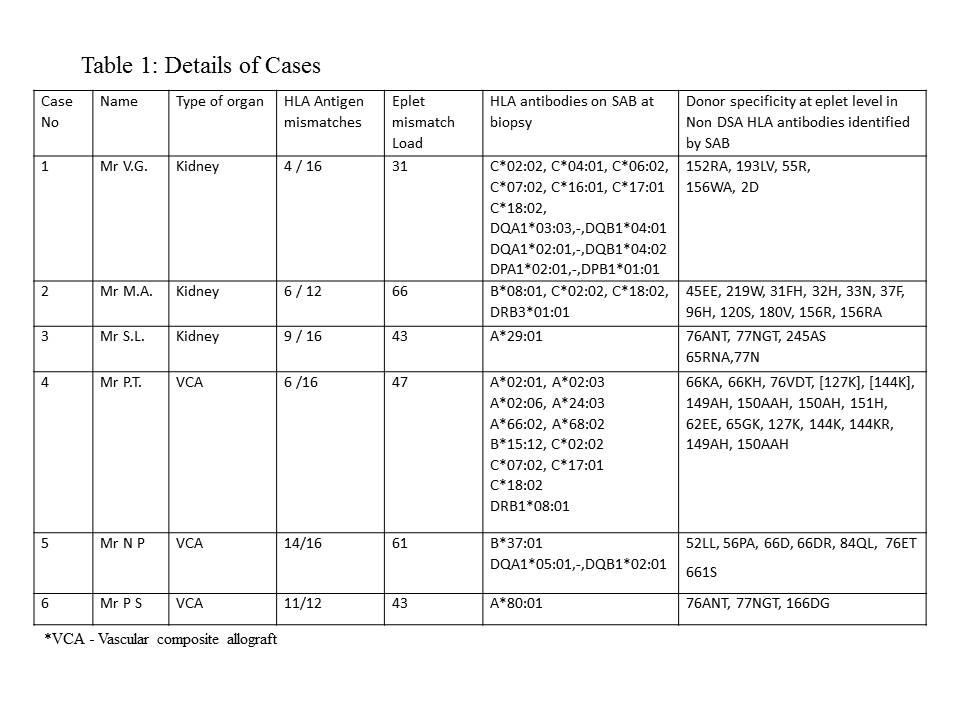
Results: There were 3 kidney transplant and 3 Vascular composite allograft recipients who had presented with biopsy proven ABMR and absence of DSAs in the circulation. One renal transplant recipient had chronic ABMR and lost his allograft. His serum never displayed any DSAs against donor HLA, but when retrospectively studied, revealed high exposition antibody verified eplets. All the six transplant recipients had developed De Novo HLA antibodies against mismatched eplets in the post transplant period. The average eplet mismatch load was 48. Presence of antibody verified eplets with high exposition were observed in all the 6 patients.
Eplet mismatches and antibody verified eplet details are displayed in the table 1.
Conclusion: Eplet mismatch load should be assessed at transplantation. Eplet mismatches confer substantial risk for formation of de novo antiody formation, episodes of ABMR and allograft loss. De-Novo antibodies against the mismatched eplets should be monitored. In cases of ABMR, antibodies against mismatched eplets can aid the diagnosis of ABMR and further post-transplant monitoring and could be used to guide post-transplant immunosuppression therapy.
