
Dr. Koçak graduated from Hacettepe University School of Medicine in 1996. He completed his residency training in Urology at Türkiye Yüksek İhtisas Hospital in 2001. He finished his transplant surgery fellowship at Northwestern University Feinberg School of Medicine in 2004. He was a faculty member and the Director of the Kidney Transplant Program at Ondokuzmayıs University School of Medicine between 2005 and 2007. He served as the Director of The Kidney and Pancreas Transplant Programs at Memorial Şişli Hospital for over a decade (2007-2018). He was promoted to associate professor in 2011 and became a full professor in 2018. He joined Koç University Hospital as the Director of the Kidney and Pancreas Transplant Programs and a faculty member in 2018. Dr. Koçak is certified by The American Society of Transplant Surgeons for Kidney and Pancreas Transplantation.
Implementing a robot-assisted kidney transplant program for transplant surgeons with no robotic surgery background: How are we doing so far?
Burak Kocak1, Serkan Sucu2, Basak Akyollu1, Emre Arpali3, Cihan Karatas1, Besir Kilicer1, Erdem Canda4, Yakup Kordan4.
1Organ Transplantation, Koc University Hospital, Istanbul, Turkey; 2General Surgery, Koc University Hospital, Istanbul, Turkey; 3Organ Transplantation, Medical College of Wisconsin, Milwaukee, WI, United States; 4Urology, Koc University Hospital, Istanbul, Turkey
Introduction: Robot-assisted kidney transplantation (RAKT) was introduced and has been performed commonly by transplant surgeons experienced in robotic surgery. Despite the demonstrated feasibility and safety of RAKT, its adoption among transplant surgeons, especially in those without prior robotic surgery experience, has been slow due to concerns over the learning curve and potential complications including the most feared graft loss avoiding its spread to new centers. In this study, we proposed a training pathway for implementing RAKT for transplant surgeons without a robotic surgery background for a safe transition.
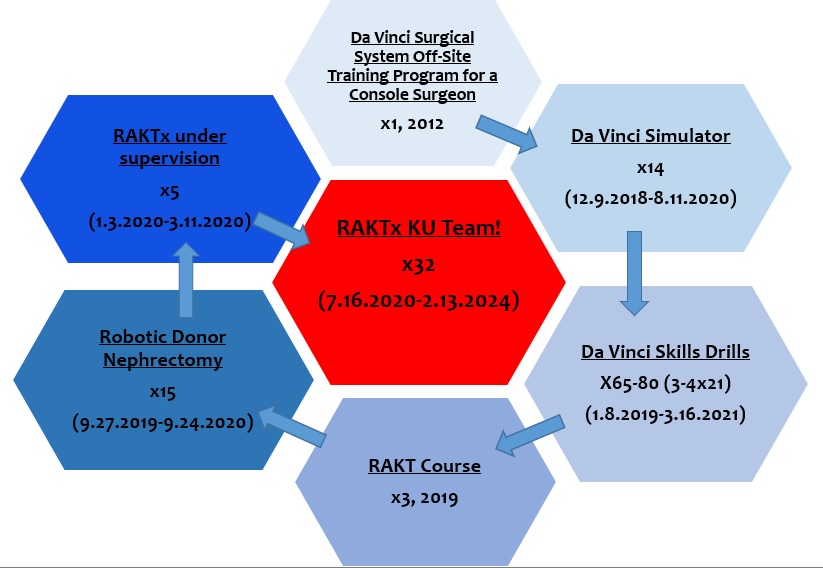
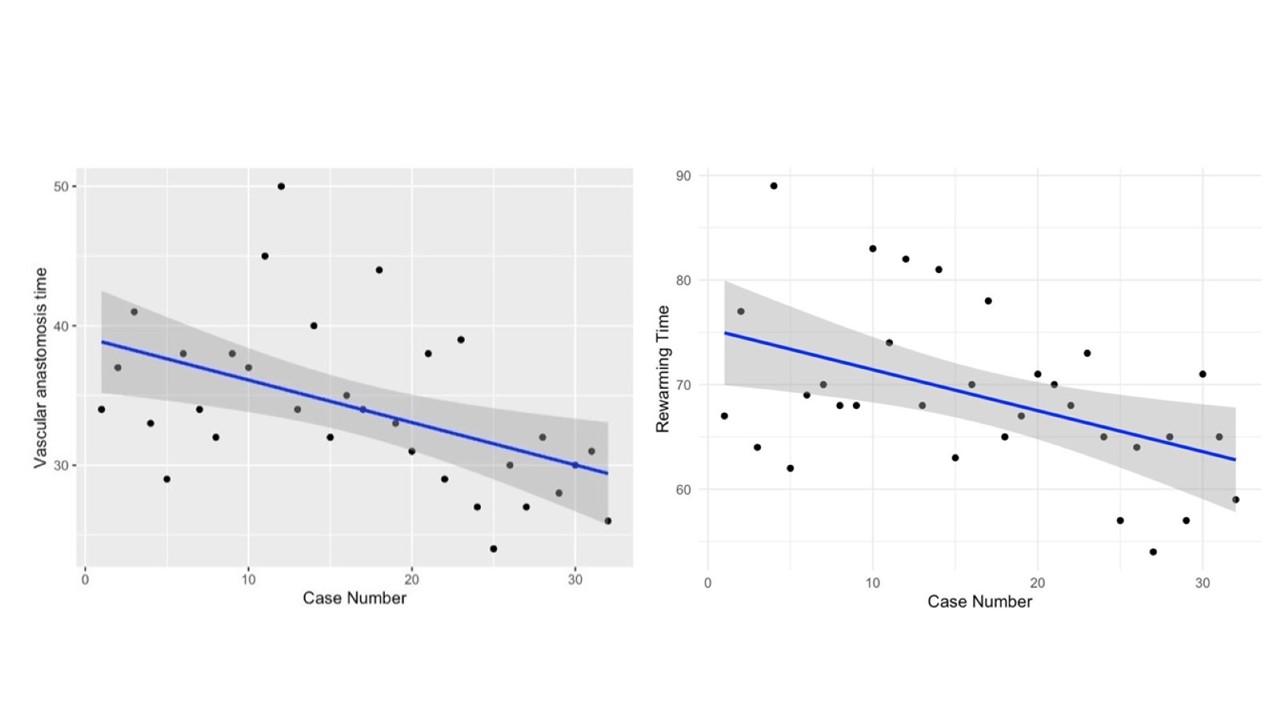
Methods: The training pathway included an off-site training program, robot simulation exercises, skill drills, attended courses, case observations and operating under the supervision of a proctor. We retrospectively analyzed RAKTs performed between January 2020 and February 2024 in our center in terms of patient and donor characteristics, indications, operative, console and rewarming times, times for vascular and ureterovesical anastomosis, postoperative complications and patient and graft survivals. Statistical analysis was performed using linear regression models to assess the learning curve's impact on analyzed times.
Results: All RAKTs were performed by the same transplant surgeon. First step was simulator training and robotic training with vascular anastomosis model followed by the hands-on RAKT training courses in a porcine model. Performing surgeon attended 3 standardized courses at different time points. The same surgeon performed 15 robot-assisted donor nephrectomies prior to RAKT. 37 RAKTs were performed. The patient request was the indication for RAKT. Recipient surgeries were performed with Da Vinci Xi with allografts procured with hand-assisted laparoscopic donor nephrectomy. First 5 cases were carried out under the supervision of expert RAKT surgeons.
The median age was 33 (range 16-58)years with median BMI of 21.5 (range 15.8-33.3). The median operative time was 396 (range 280-490)min. The median console and rewarming times were 232 (range 155-360)min, 68 (range 54-89)min, respectively. The median total vascular anastomosis time was 33 (range 24-50)min, while the median ureterovesical anastomosis time was 27 (range 16-60)min. Statistical analysis showed that the learning curve excluding the first five supervised cases for vascular anastomosis and rewarming times were significantly improved with increased experience.
Postoperative complications were minor, with only one patient requiring reoperation due to small bowel obstruction. There was no delayed graft function. Overall patient and graft survival rates were 100% in the median follow-up period of 31 (range 1-51) months.
Conclusions: We demonstrated that the RAKT implementation model for transplant surgeons without prior robotic surgery experience is feasible and can achieve favorable outcomes following a structured training pathway.
[1] Robotics
[2] Kidney
[3] Transplantation
[4] Robot assisted kidney transplantation
