
Simultaneous pancreas and kidney transplantation from a small pediatric donor with ipsilateral implantation over aortic cuff
Nasika Venkata Kanaka Naga Karthik1, Ashish Sharma1, Deepesh B Kenwar1, Sarbpreet Singh1, Jasmine Sethi2, Abhilash Tirkey1, Bharat Bhushan1, Sanjeev Chauhan1, Sai Praneeth Reddy1.
1RENAL TRANSPLANT SURGERY, PGIMER, CHANDIGARH, India; 2NEPHROLOGY, PGIMER, CHANDIGARH, India
Introduction: There are very few cases reported of simultaneous pancreas and kidney transplants from paediatric donors owing to the lack of knowledge and skill. This case focuses on such paediatric donors with carrel patch implantation of pancreas with ipsilateral kidney transplantation
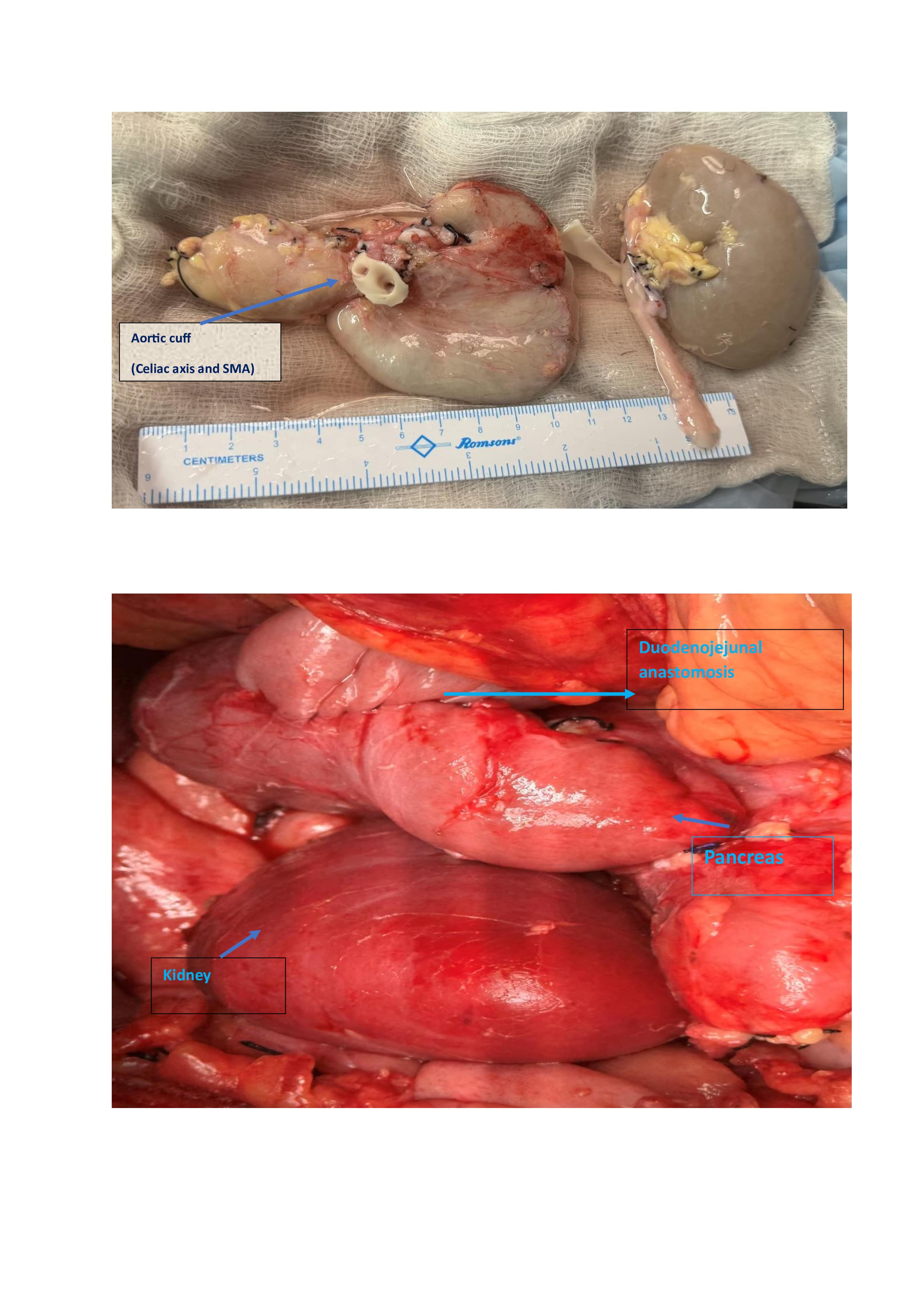
Case Description: A 24-year-old male with type I diabetes and end stage renal disease on maintenance haemodialysis for 4 years had undergone simultaneous pancreatic kidney transplantation from a paediatric 5-year-old donor. The donor child had a history of fall with irreversible head injury. The child was declared brain dead and multiorgan retrieval was done. There were steady vitals with minimal inotropic support and organs had good predonation function. Pancreas was retrieved en block with spleen and entire aortic cuff containing celiac axis and superior mesenteric artery was taken. Heart, Liver and both kidneys were also retrieved. The organs were of excellent quality macroscopically (non-fatty). Virtual cross match was done with potential recipient. Antithymocyte globulin induction was prior to surgery. Right side ipsilateral placement of pancreas over the aortic cuff and kidney done. Pancreas aortic cuff anastomosed with recipient aorta and portal vein anastomosed to inferior vena cava. Left (donor) kidney was placed below pancreas with artery anastomosed to common iliac artery, renal vein to external iliac vein and ureter to bladder (extravesical approach). There was good perfusion of organs with brisk diuresis and fall in blood sugars. Duodenum of donor pancreas was anastomosed with jejunum for drainage. The total ischemic time was 365 min.
Triple immunosuppressive regimen (tacrolimus, mycophenolate and steroids) and anticoagulation (Heparin infusion) were given postoperatively. He had mild peri graft haematoma and melena. Anticoagulation was stopped and upper gastrointestinal endoscopy showed normal findings and subsequently resolved without any intervention. There was no increment in serum and drain fluid amylase/lipase. There was good urine output with steady fall in creatinine with 1.1 mg/dl and tacrolimus level of 11.4ng/ml at discharge. On three months follow up, his blood sugars were in the normal range(90-170mg/dl) and creatinine value of 1.2mg/dl with good dual graft function.
Conclusion: With limited organs, paediatric donors provide effective source to the scarcity of organs. Although technically challenging, direct pancreas implantation using aortic cuff removes the vessel reconstruction with graft and kidney implantation on the same side limits further dissection. This case also shows good sugar control and kidney function in adult recipients by pediatric organ mass (islet and nephron mass) implicating value of such donation.
[1] Simultaneous pancreas and kidney transplantation
[2] Small pediatric donor
[3] Type I diabetes mellitus
[4] Aortic cuff implantation
