Cortical ribbon sign in a liver transplant recipient with hepatic encephalopathy
Deniz Sivrioglu1, Seda Kibaroglu2, Fatma Irem Yesiler1, Helin Sahinturk1, Pinar Zeyneloglu1, Mehmet A. Haberal3.
1Department of Anaesthiology and Reanimation, Baskent University, Ankara, Turkey; 2Department of Neurology, Baskent University, Ankara, Turkey; 3Department of General Surgery, Division of Transplantation, Baskent University, Ankara, Turkey
Introduction: The clinical presentations and magnetic resonance imaging (MRI) findings of hepatic encephalopathy (HE) may mimic those observed in Creutzfeldt-Jakob disease (CJD) (1). This case report describes a liver transplant recipient who demonstrated the cortical ribbon sign on MRI post-transplantation, a sign traditionally associated with CJD, but herein attributed to HE.
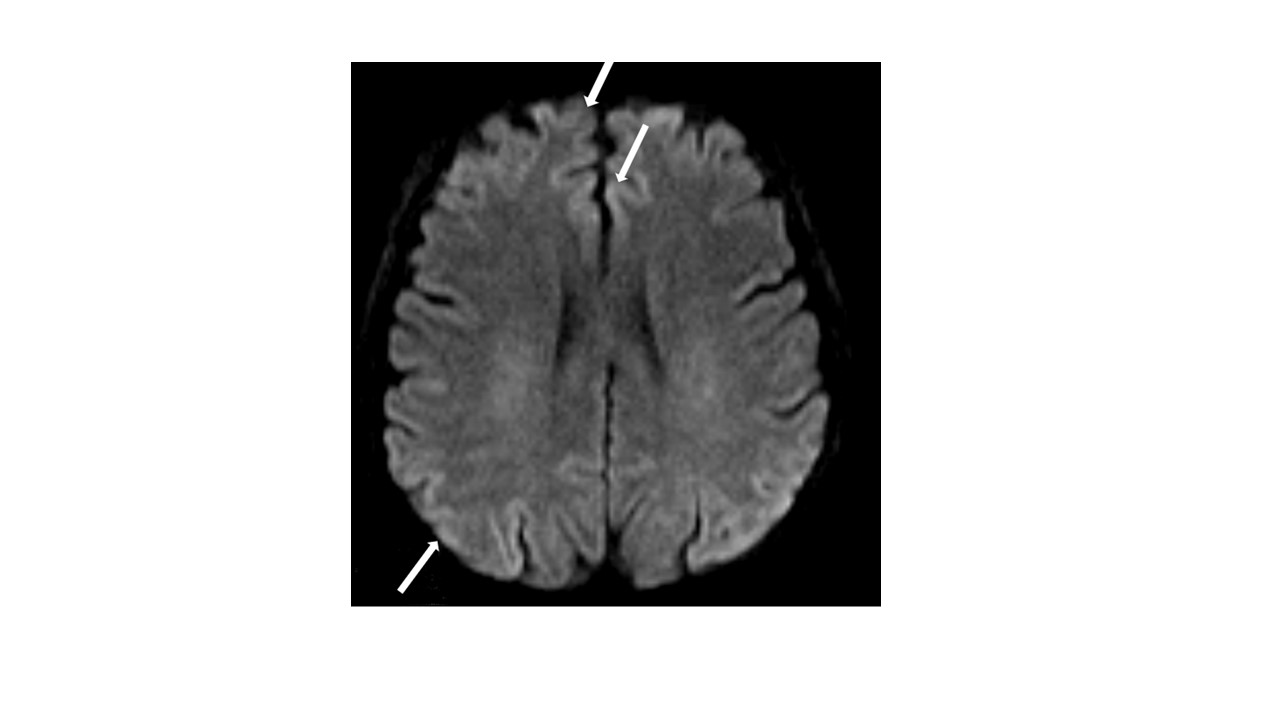
Case Presentation: A 54 -year-old female patient was admitted to intensive care unit (ICU) after a living donor liver transplantation (LDLT) at early postoperative period. Her medical history had diabetes mellitus, cryptogenic cirrhosis, portal vein thrombosis, hepatorenal syndrome, and recurrent hepatic encephalopathy episodes and TIPS. Her MELD and Child Pugg scores were 19 and 11C, respectively. At ICU admission APACHE-II score was 8, she was intubated and needed cardiovascular support with vasopressors and inotropes. A total of 24 sessions of therapeutic plasma exchange were applied for delayed graft response due to small for size syndrome and continous renal replacement therapy (CRRT) was applied due to stage 3 acute kidney injury. On the 8th day of invasive mechanical ventilation, 48 hours after sedation weaning, there was no awareness and GCS was 8. Cerebral MRI DWI showed a ribbon-like signal hyperintensity of cerebral cortical gyri (cortical ribboning) of the right predominant bilateral frontal, parietal, and occipital lobes, known as the cortical ribbon sign (Figure-1). Lumbar puncture could not be performed due to thrombocytopenia and EEG could not be performed due to hemodynamic instability. CJD was not considered in the patient because she had no history of prion exposure and her conscious improved without CJD treatment on 10th day of ICU. Therefore, it was considered that the patient had hepatic encephalopathy due to her current metabolic state. The patient died on the 14th day of ICU admission due to sepsis related to multidrug-resistant bacterial infection and respiratory syncytial virus.
Conclusion: Although the cortical ribbon sign is characteristic of CJD, it should be kept in mind that it can also be seen in clinical conditions such as infection, hypoxia, electrolyte disturbances and hepatic encephalopathy (2,3). In a liver transplant recipient with HE who do not undergo further examination, the patient's medical history and clinical examination may help for the differential diagnosis of cortical ribbon sign on MRI.