Systemic improvements in a single-center simultaneous pancreas and kidney transplant program
Lucia Alfaro Villanueva1, Roberto Meirelles Junior1, Adriano Miziara1, Lucio Requiao Moura1, Helio Tedesco-Silva1, Jose Medina-Pestana1.
1Pancreas and kidney transplant program, Hospital do Rim e Hipertensão, Sao Paulo , Brazil
Background: Simultaneous pancreas and kidney (SPK) transplantation faces several donor, recipient, surgical, clinical, and immunological challenges.
Aim: To identify prognostic factors and compare 12-month patient survival after SPK according to 5 eras during the last 20 years.
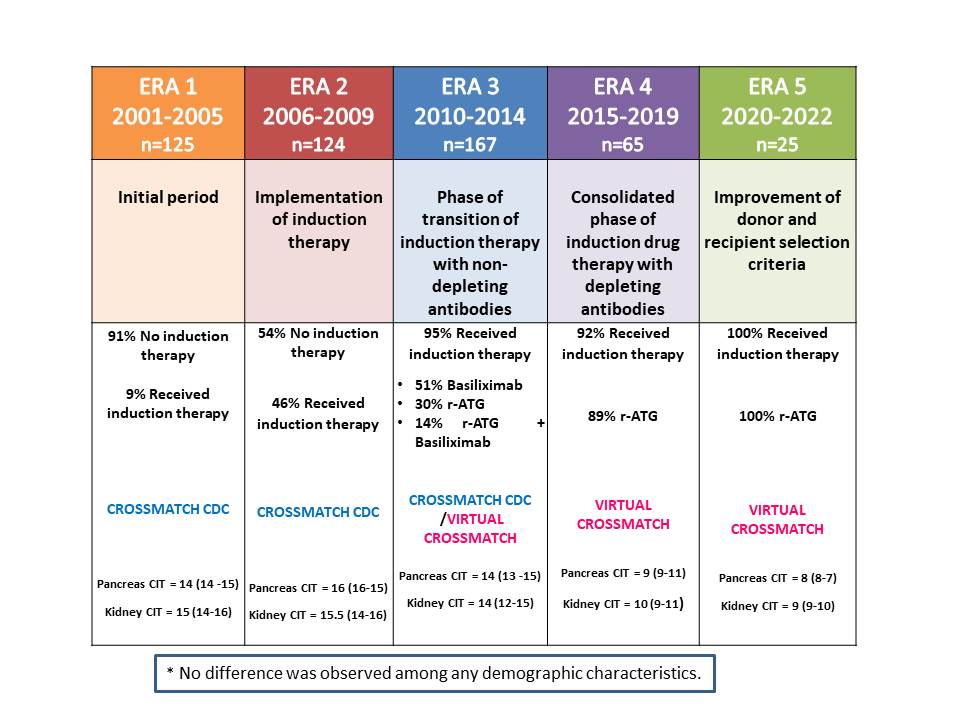
Methodology: This is a single-center, retrospective, observational study that enrolled 506 patients undergoing consecutive SPK transplant between January 2001 and April 2022. The cohort was divided into 5 eras according to the predominant change in the institutional protocol: Era 1 (2001-2005) the initial period; Era 2 (2006-2009) the implementation of induction therapy with non-depleting antibodies; Era 3 (2010-2014) transition to depleting antibodies and the use of virtual crossmatch; Era 4 (2015-2019) induction therapy using depleting antibodies; Era 5 (2020-2022) the improvement of the donor and recipient selection criteria. The primary outcome was patient survival according to the era. The secondary outcome was pancreas and kidney graft survival according to the era. (Table 1)
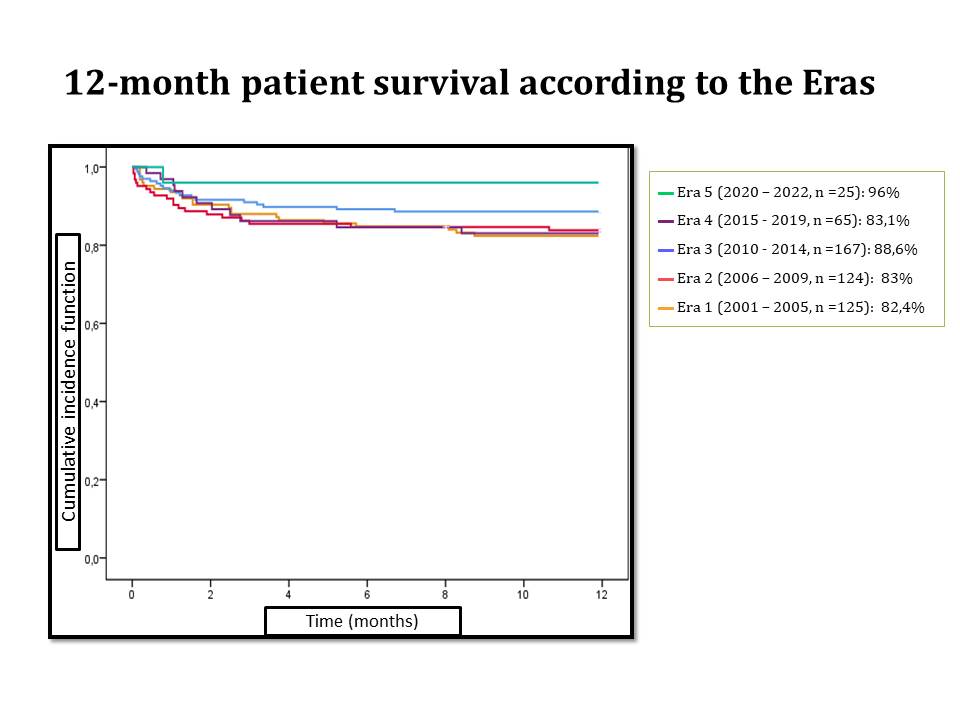
Results: Patient 12-month survival was 82.4% (Era 1, n=125) vs. 83% (Era 2, n=124) vs. 88.6% (Era 3, n=167) vs. 83% (Era 4, n=65) vs. 96% (Era 5, n=22) (p=0.315), (Figure 1). Pancreas 12-month graft survival improved over time, from 78.4% (Era 1) vs. 75% (Era 2) vs 76.7% (Era 3) vs. 81.4% (Era 4) vs 87.8% (Era 5) (p=0.639). Kidney 12-month graft survival was 80% (Era 1) vs. 83.1 (Era 2) vs 87.4% (Era 3) vs. 87.3% (Era 4) vs 100% (Era 5) after SPKT (p=0.101).
Conclusion: This analysis confirms that stepwise improvements in the institutional protocol, including the use of induction therapy, reduction of the cold ischemia time, the implementation of virtual crossmatch and the more restrict donor and recipient selection criteria were associated with improvement in patient and graft survival after SPK transplantation.
[1] simultaneous pancreas and kidney transplantation
[2] patient survival
[3] systemic improvements
[4] pancreas graft survival
[5] kidney graft survival
