Socioeconomic disadvantage, all-cause and cause-specific mortality in patients treated with maintenance dialysis: A causal mediation analysis of geographical inequity and multimorbidity
Farzaneh Boroumand1,2,3, Wai H Lim4,5, Shuvo Bakar1, Ryan Gately1,2, Pedro Lopez4,5, Dharshana Sabanayagam1,2, Anita Van Zwieten1,2, Lin Zhu1, Germaine Wong1,2, Armando Teixeira-Pinto1,2.
1Sydney School of Public Health, University of Sydney, Sydney, Australia; 2Center for Kidney Research, Kids Research Institute , The Children’s Hospital at Westmead, Sydney, Australia; 3School of Mathematical and Physical Sciences, Macquarie University, Sydney, Australia; 4Pleural Medicine Unit, Institute for Respiratory Health, Perth, Australia; 55Medical School, Faculty of Health & Medical Sciences, University of Western Australia, Perth, Australia
Introduction: The social gradient of health is significant and persuasive in patients with kidney failure but the causal pathways of this relationship are unknown. We aimed to assess the mediating effects of multimorbidity and geographical remoteness in the SES-death associations.
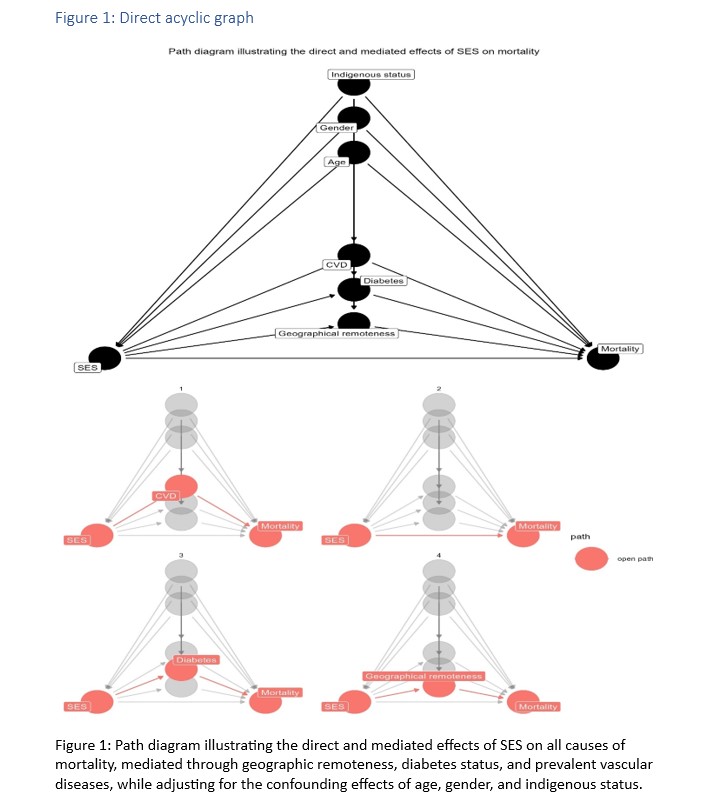
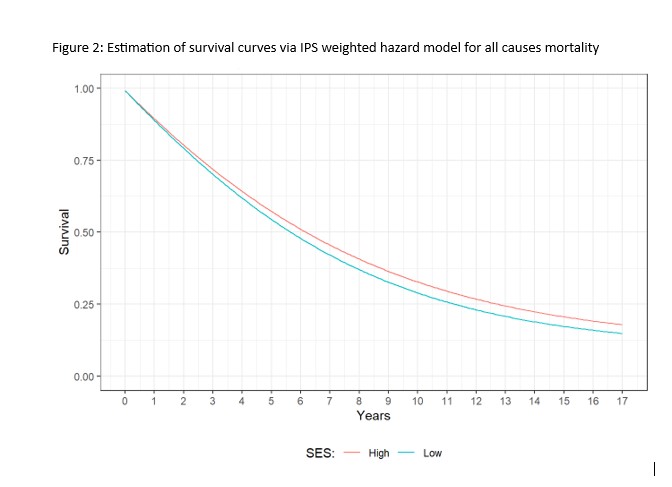
Methods: This cohort study included all patients with kidney failure aged 18 years or over who commenced dialysis in Australia between 2005 and 2019. Using data from the Australia and New Zealand Dialysis and Transplant (ANZDATA) registry, the causal effect of SES on all-cause and cause-specific death was analysed using the inverse probability stabilised weighting (IPSW) approach. We then conducted a mediation analysis to explore the mediating effects of geographical remoteness, diabetes status and cardiovascular disease (CVD) on the association between lower SES, all-cause and cause-specific death.
Results: We included a total of 35,239 incident patients with kidney failure who initiated dialysis in Australia between 2005 and 2019, with a median (IQR) follow-up period of 4.0 (2.0, 7.1) years. Of these, 20,597 (54%) patients were from low SES backgrounds. Compared to patients from higher SES backgrounds, those from lower SES experienced a 1.2-fold increased risk of death (HR (95%CI) = 1.2 (1.1-1.3)). The proportions of the effect between SES and all-cause mortality on dialysis mediated by geographical remoteness, CVD and diabetes were 30.5%, 8.6%, 15.5%, respectively, accounting for 54.6% of the total effect, while SES explained 45.4% of the total effect, directly. Compared to patients from high SES backgrounds, those from lower SES backgrounds experienced a higher risk of CVD-related mortality, HR (95%CI) = 1.3 (1.2-1.5). However, geographical remoteness did not mediate the effect of SES on CVD-related mortality. On the contrary, the effect of SES on CVD-related mortality was mediated by CVD and diabetes, with CVD and diabetes contributing 10.8%, and 18.9%, that is 29.7% of total effect, while the direct effect of SES accounted for 70.3% of the total effect. Patients from low SES backgrounds experienced a higher risk of infection-related mortality compared to those from higher SES backgrounds, HR (95%CI) =1.1(1.0-1.3). This effect was mediated through CVD and diabetes, with CVD and diabetes contributing, 8.3% and 19.5%, that is 24.1% of total effect, while the direct effect of SES accounting for 75.9% of the total effect.
Conclusion: Geographical remoteness, diabetes, and vascular disease mediated over 50% of the association between low SES and all-cause mortality in patients treated with dialysis. Therefore, effective strategies to treat and manage these comorbidities aggressively, and approaches to improve geographical inequity may reduce the health disparities observed in this vulnerable population.
The authors acknowledge the University of Sydney HPC service at The University of Sydney for providing resources that have contributed to the research results reported within this paper.
[1] Dialysis
[2] Kidney Failure
[3] Causal mediation analysis
[4] Infection related mortality
[5] Cardiovascular related mortality
[6] Geographical inequity
[7] Socioeconomic disadvantage
