The national landscape of kidney transplantation among presumed unauthorized immigrants in the United States
Mara McAdams DeMarco1,2, Gayathri Menon1, Garyn Metoyer1, Yiting Li1, Yusi Chen1, Sunjae Bae1, Brian P Lee3, Pablo C Loarte-Campos4, Babak Orandi1,4, Dorry L Segev1,2.
1Department of Surgery, New York University Grossman School of Medicine, New York, NY, United States; 2Department of Population Health, New York University Grossman School of Medicine, New York, NY, United States; 3Division of Gastrointestinal and Liver Diseases, Keck School of Medicine of University of Southern California, Los Angeles, CA, United States; 4Department of Medicine, New York University Grossman School of Medicine, New York, NY, United States
Introduction: Unauthorized immigrants may experience challenges in accessing kidney transplantation (KT) due to healthcare access, socioeconomic, and cultural barriers. Understanding the national landscape and impact of state policies covering KT for unauthorized immigrants is needed to inform policy changes. Therefore, we characterize the national and state-level KT landscape for presumed unauthorized immigrants (PUI) and permanent residents (residents hereafter) relative to citizens.
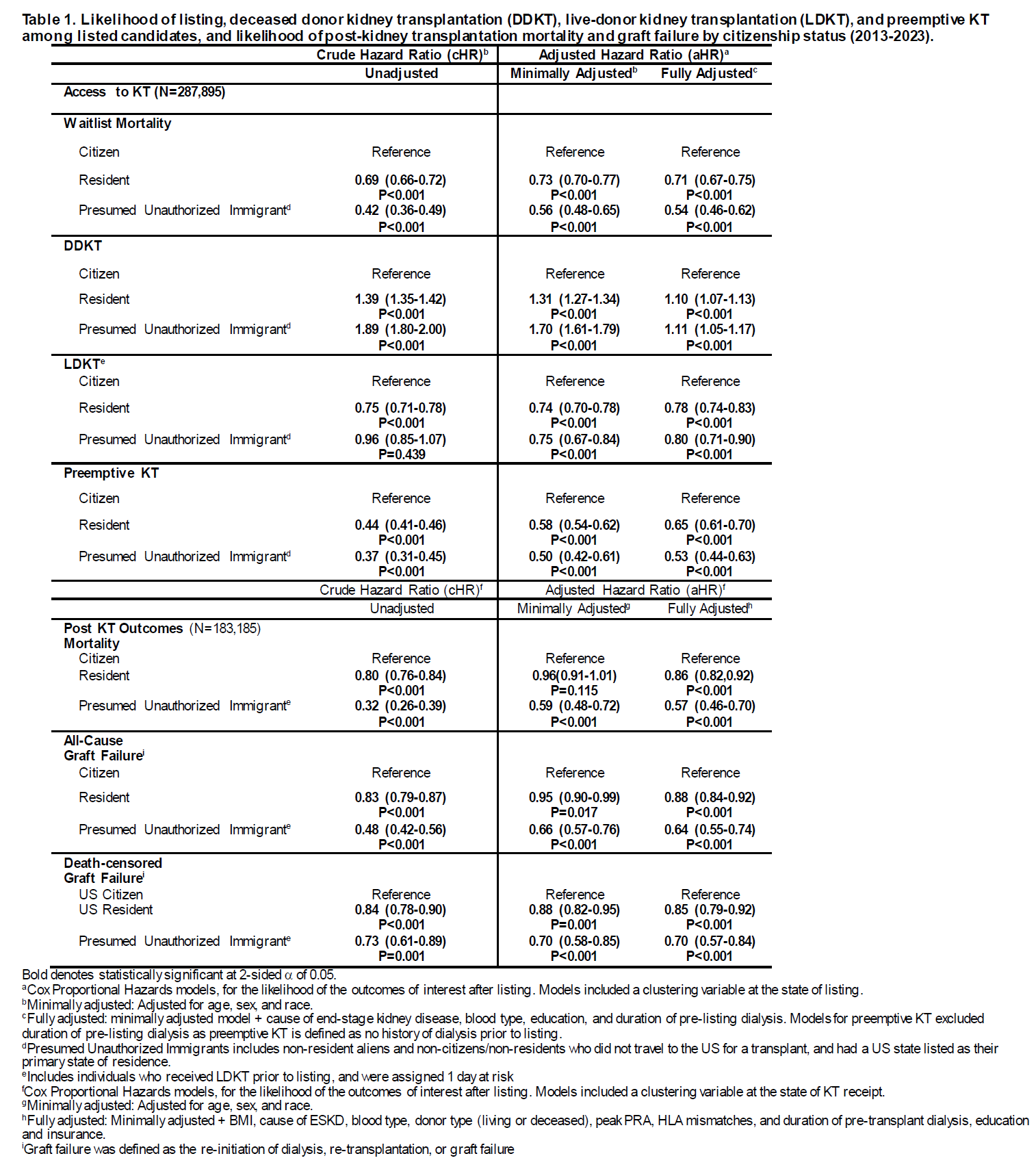
Method: We used data from the national registry to identify adults (age³18 years) listed for their first KT (N=287,895) and first KT recipients (N=183,185) (2013-2023). We used negative binomial regression models to quantify the incidence of listing over time among PUI. We then used cause-specific hazards models to calculate the adjusted hazard ratio (aHR) of waitlist mortality, deceased-donor KT [DDKT], live-donor KT [LDKT], preemptive KT and post-KT outcomes (mortality/graft failure) by citizenship category. Lastly, in states where policies changes were made to provide KT coverage for PUI during the study period (Illinois, Massachusetts, and Minnesota), we used similar methods to quantify the adjusted incidence rate ratio (aIRR) of listing and adjusted hazard ratio of KT pre- and post-policy by citizenship status.
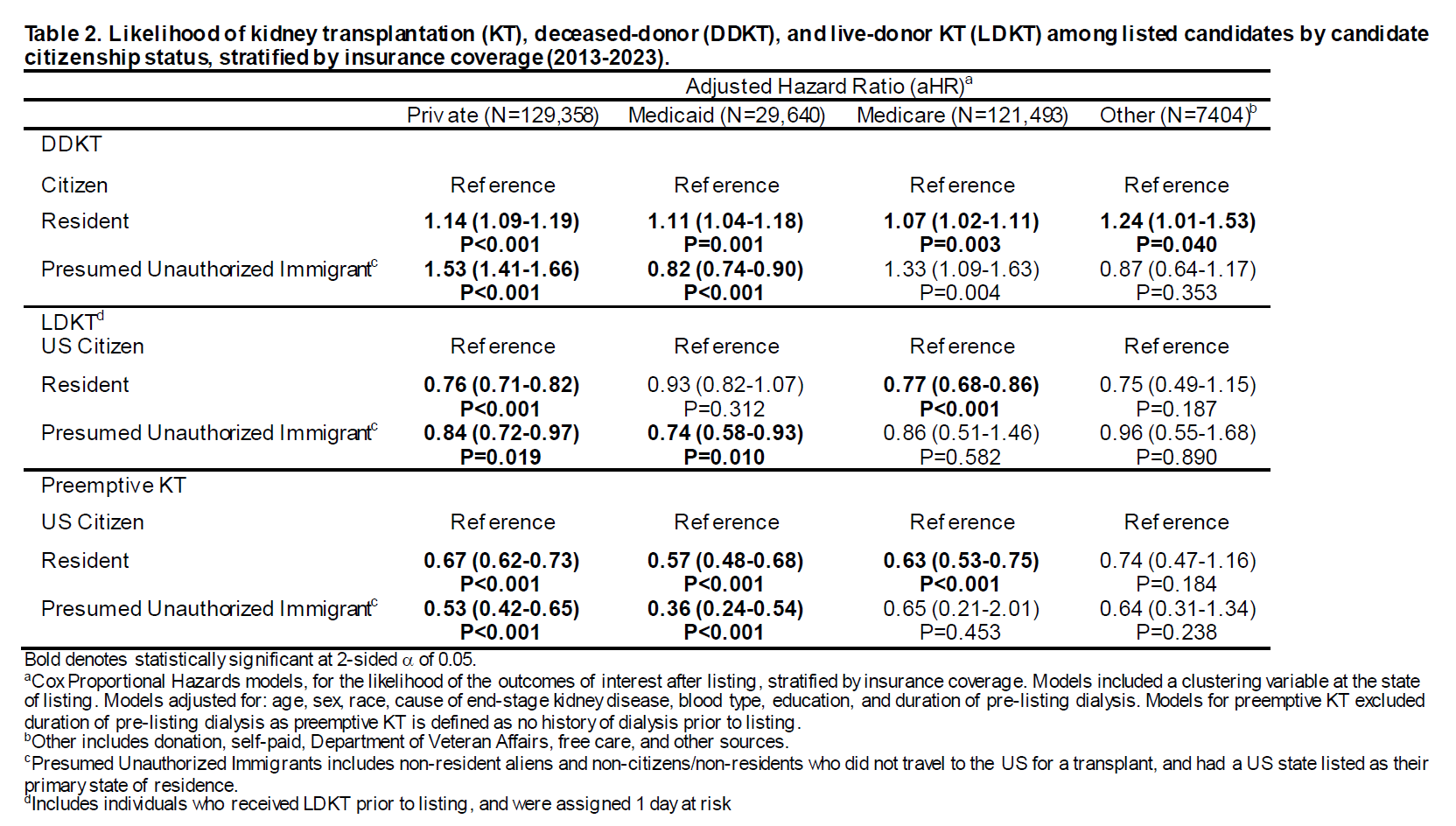
Results: The proportion of PUI listed increased over time (2013:0.9% vs. 2023:1.9%); however, after accounting for case mix and waitlist size, this difference attenuated. PUI experienced a lower risk of waitlist mortality (aHR=0.54, 95%CI:0.46-0.62); they were more likely to obtain DDKT (aHR=1.11, 95%CI:1.05-1.17) but less likely to obtain LDKT (aHR=0.80, 95%CI:0.71-0.90) or preemptive KT (aHR=0.53, 95%CI:0.44-0.63). However, higher access to DDKT among PUI was driven by those with private insurance, while those with Medicaid were less likely to obtain DDKT. 1.2% of KT recipients were PUI; they were less likely to experience post-KT mortality (aHR=0.57, 95%CI:0.46-0.70) and graft failure (aHR=0.70, 95%CI:0.57-0.84). Similar findings for access to KT and post-KT outcomes were obtained for residents. After policy changes in 3 states, PUI were more likely to be listed (IRR=2.18, 95%CI:1.13-4.20; P=0.021), but their likelihood of DDKT or LDKT was unchanged (all Pinteraction>0.05).
Conclusion: This is the first comprehensive national landscape of KT for unauthorized immigrants, which highlights the challenges faced by this population. The findings from the 3 states with policy change may inform national policies aimed at improving equity in transplantation among PUI.
This work was supported by grant number R01AG077888 (PI: McAdams-DeMarco) from the National Institute on Aging (NIA). In addition, co-authors are also supported by the following grant numbers: K02AG076883 (PI: McAdams-DeMarco), and R01AG055781 (PI: McAdams-DeMarco) from the National Institute on Aging (NIA); R01DK114074 (PI: McAdams-DeMarco), R01DK120518 (PI: McAdams-DeMarco) from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK); and K24AI144954 (PI: Segev) from the National Institute of Allergy and Infectious Diseases (NIAID). Additionally, the funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript or the decision to submit.
[1] unauthorized immigrants
[2] kidney transplantation
[3] post-transplantation outcomes
[4] citizenship status
