
The combination of TTV viral load and BKV-neutralizing antibody titers aids in stratifying the risk of BKV viremia
Ilies Benotmane1, Morgane Solis2, Samira Fafi-Kremer2, Sophie Caillard1.
1Service de Néphrologie-Dialyse-Transplantation, Hôpitaux Universitaires de Strasbourg, Strasbourg, France; 2Service de Virologie, Hôpitaux Universitaires de Strasbourg, Strasbourg, France
Introduction: Torque teno virus (TTV) viral load is an emerging marker of immunosuppression, yet its correlation with BKPyV replication remains uncertain. Our previous findings underscored that a neutralizing antibody titer (NABS) <4 log10 against the donor BKPyV strain heightens the risk of BKPyV viremia, while patients with a titer >4 log10 are less susceptible. This study investigates the relationship between TTV viral load and BKPyV replication based on the anti-BKPyV NABs titer.
Methods: In a retrospective cohort of 76 kidney transplant recipients, NABS were measured at transplantation, while the TTV viral load was assessed one month post-transplant (M1). BKPyV viremia was monitored throughout the initial post-transplant year.
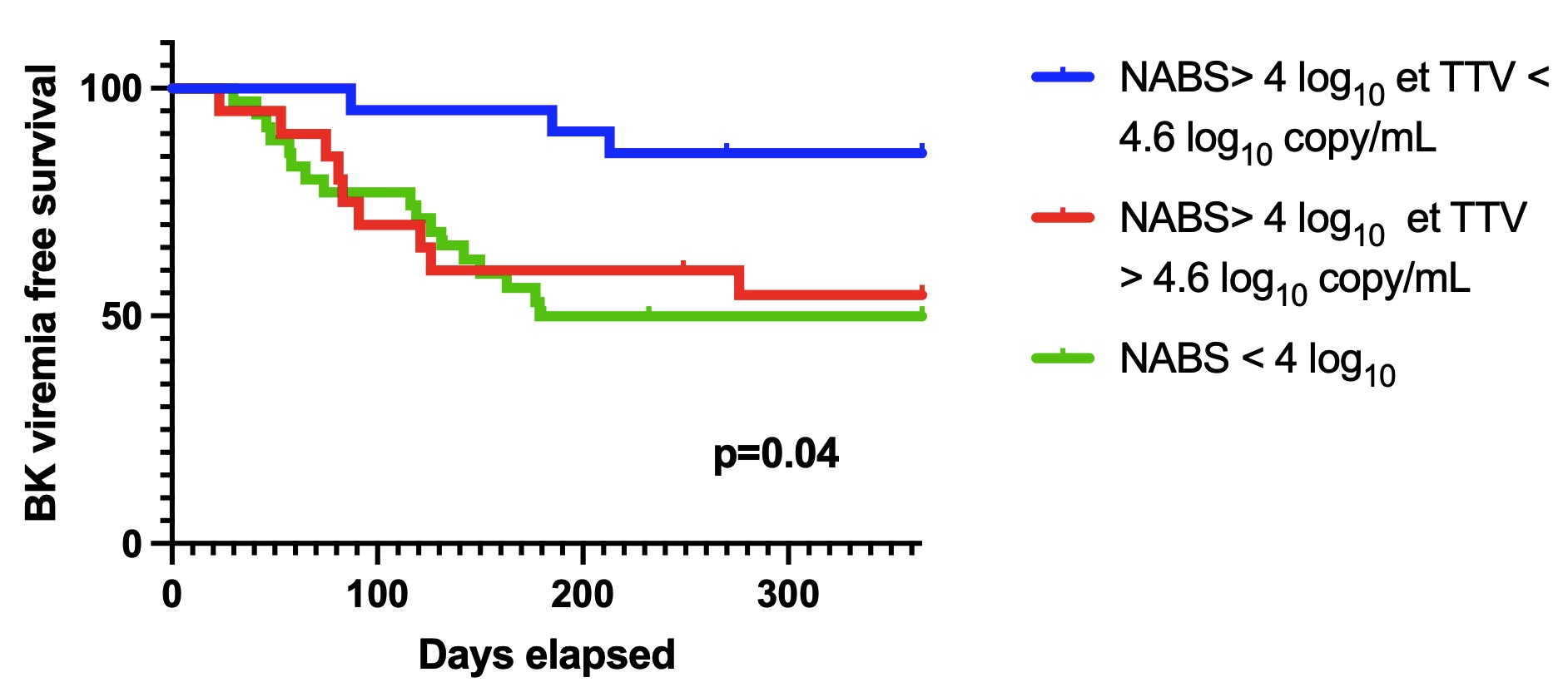
Results: The median age was 56 years with an IQR of 49-65.7. Regarding immunosuppressive therapy, 58% were under anti-human thymocyte immunoglobulin, and 67% were under tacrolimus, all under MMF. At one year, BKPyV viremia occurred in 18 out of 35 patients with NABS < 4 log10 compared to 13 out of 41 with NABS > 4 log10 (p = 0.06). Overall, the median TTV viral load showed no association with BKPyV viremia (5.2 log10 vs. 4.4 log10 copies/ml, p = 0.07). However, in the "NABS > 4 log10" group, patients with BKPyV viremia exhibited a higher TTV viral load (5.4 log10 vs. 4.3 log10 copies/ml, p = 0.01), while the immunosuppressive regimen, residual levels of calcineurin inhibitors, and the area under the curve of MMF at M1 were similar, regardless of BK viremia. Conversely, in the "NABS < 4 log10" group, BKV replication was not associated with a higher TTV viral load (4.8 log10 vs. 4.9 log10 copies/ml, p = 0.72). NABS titer and TTV viral load stratified our population into three distinct risks of BKPyV replication (Figure 1). Interestingly, the median time to the onset of viremia is longer in the group "NABS > 4 log10 and TTV viral load > 4.6 log10" compared to the two other groups, with medians of 191 vs 91 (p=0.03).
Conclusions: Patients with a high anti-BKPyV-NABS titer and low TTV viral load had the lowest risk of BKPyV replication, suggesting the necessity for adequate humoral and cellular immunity to prevent BKPyV in kidney transplant recipients.
[1] TTV
[2] Kidney transplant organ
[3] BKPyV
