Delayed initiation or reduced initial dose of calcineurin-inhibitors for kidney transplant recipients: A systematic review and meta-analysis
Laia Oliveras1,2, Edoardo Melilli1,2, Sergi Codina1,2, Ana Coloma1,2, Àlex Favà1, Anna Manonelles1,2, Núria Lloberas2, Carlos Couceiro1,2, Josep M Cruzado1,2, Núria Montero1,2.
1Nephrology, Hospital Universitari de Bellvitge, L'Hospitalet de Llobregat, Spain; 2Nephrology and Transplantation, Biomedical Research Institute (IDIBELL), L'Hospitalet de Llobregat, Spain
Introduction: Delayed graft function (DGF) is more common in donors after cardiac death, especially expanded criteria donors and those with longer cold ischemia time, older or with an increased serum creatinine. There is no agreement on the optimal immunosuppressive approach in patients at increased risk of DGF, with strategies including a delayed introduction of calcineurin inhibitors (CNI) or initial low dose CNI. Our aim was to evaluate the benefits and harms of delayed initiation of CNI or reduced CNI dose as initial immunosuppression therapy for kidney transplant (KT) recipients at high risk of DGF.
Method: We searched the Cochrane Kidney and Transplant Register of Studies up to 07 March 2023 through contact with the Information Specialist using search terms relevant to this review. Studies in the Register are identified through searches of CENTRAL, MEDLINE, and EMBASE, conference proceedings, the International Clinical Trials Register (ICTRP) Search Portal, and ClinicalTrials.gov. We included all randomized controlled trials (RCTs) and quasi-RCTs evaluating early vs delayed initiation of CNI or reduced vs standard initial dose of CNI in kidney transplant (KT) recipients at high risk of DGF. Three authors independently assessed study eligibility, and two assessed the risk of bias, certainty of evidence, extracted the data, and performed the analysis. Results were reported as risk ratios with 95% confidence intervals for dichotomous outcomes and as mean difference with 95% CI for continuous outcomes. Statistical analysis was performed using the random-effects model. Risk of bias was assessed with RoB2 and the certainty of the evidence according to GRADE methods.
Results: Thirteen studies were included (2386 randomized participants). Incidence of DGF (RR 1.09, 95% CI 0.89 to 1.32; I2= 18%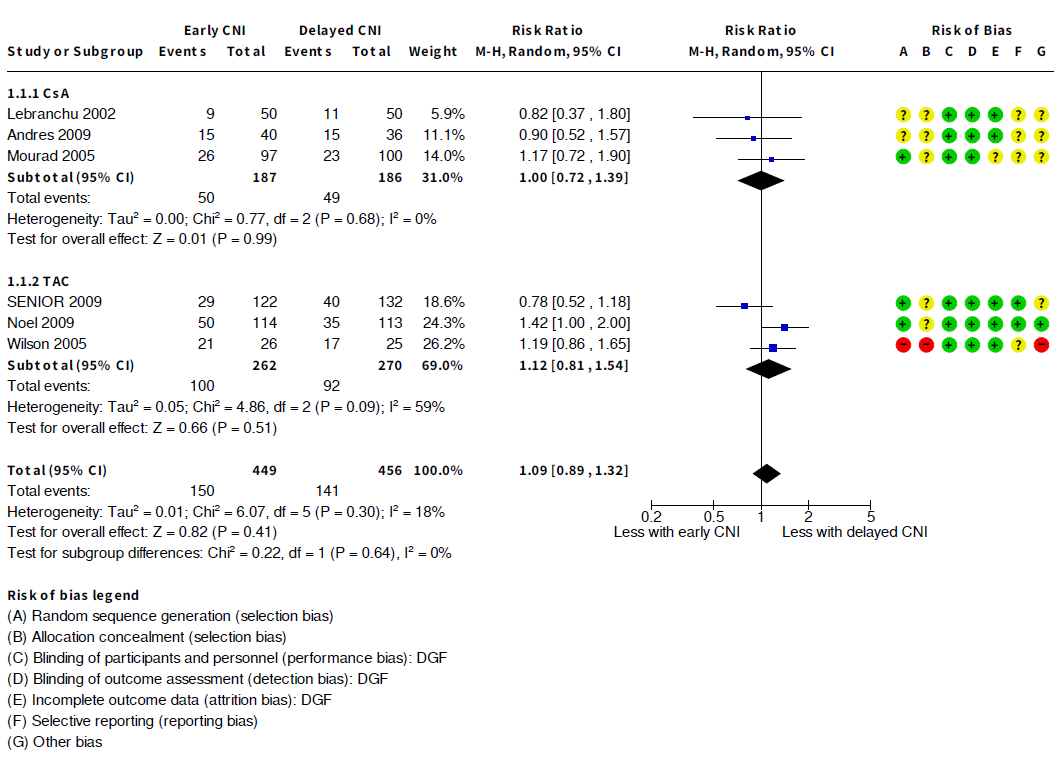
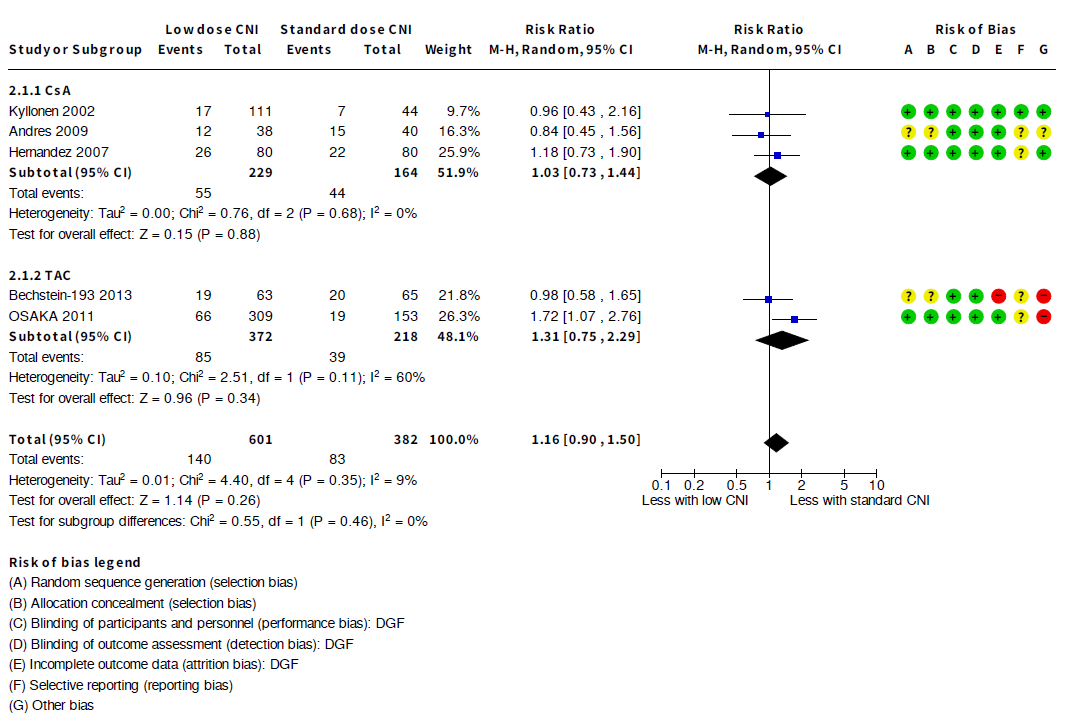 ) and acute rejection (RR 0.98, 95% CI 0.72 to 1.33; I2= 54%) were similar between early and delayed introduction of CNI, as well as between low vs standard dose of CNI (DGF: RR 1.16, 95% CI 0.90 to 1.50; I2= 9%; acute rejection: RR 0.70, 95% CI 0.43 to 1.14; I2= 58%). There were also no differences in secondary outcomes such as graft function, graft loss, risk of death, or infection.
) and acute rejection (RR 0.98, 95% CI 0.72 to 1.33; I2= 54%) were similar between early and delayed introduction of CNI, as well as between low vs standard dose of CNI (DGF: RR 1.16, 95% CI 0.90 to 1.50; I2= 9%; acute rejection: RR 0.70, 95% CI 0.43 to 1.14; I2= 58%). There were also no differences in secondary outcomes such as graft function, graft loss, risk of death, or infection.
Conclusion: In patients at high risk of DGF, the strategy of delaying CNI introduction or starting at a lower dose does not reduce the risk of DGF.
[1] immunosuppression
[2] kidney transplant
[3] delayed graft function
[4] calcineurin-inhibitor
[5] delayed initiation
