
Does de novo malignancy increase the risk of rejection in kidney transplant recipients?
Erol Demir1, Mevlut Tamer Dinçer2, Cebrail Karaca2, Cansu Erel3, Latif Karahan3, Aslihan Pekmezci2, Sinan Trabulus2, Nurhan Seyahi2, Aydin Turkmen3.
1Transplant Immunology Research Center of Excellence, Koç University, Istanbul, Turkey; 2Division of Nephrology, Department of Internal Medicine, Cerrahpaşa Faculty of Medicine, Istanbul University Cerrahpaşa, Istanbul, Turkey; 3Division of Nephrology, Department of Internal Medicine, Istanbul Faculty of Medicine, Istanbul University, Istanbul, Turkey
Introduction: Kidney transplant recipients face a significantly higher risk of developing de novo malignancies, two to three times greater than dialysis patients. However, there is a lack of information regarding whether allograft rejection increases in kidney transplant recipients with malignancies. In these cases, it remains uncertain whether reducing immunosuppression leads to a heightened risk of allograft rejection. This study explores allograft rejection and the associated risk factors in kidney transplant recipients who develop de novo malignancies.
Methods: This retrospective case-cohort study was conducted at two kidney transplantation centers. Inclusion criteria encompassed adult patients who underwent kidney transplantation between 1986 and 2020 and developed de novo malignancies. For each patient with malignancy, a matching kidney transplant recipient was selected as a control using the nearest neighbor matching method, taking into account the post-transplant follow-up period. The outcomes were biopsy-confirmed allograft rejection, mortality, and death-censored allograft loss.
Results: Out of the 2,750 medical records reviewed, 267 kidney transplant recipients (9.7%) were found to have biopsy-confirmed malignancies. These patients had a median age of 60 years (IQR25-75, 51-66), with 177 of them being men (66.3%). The median post-transplant follow-up duration was 218 months (IQR25-75, 153-290).
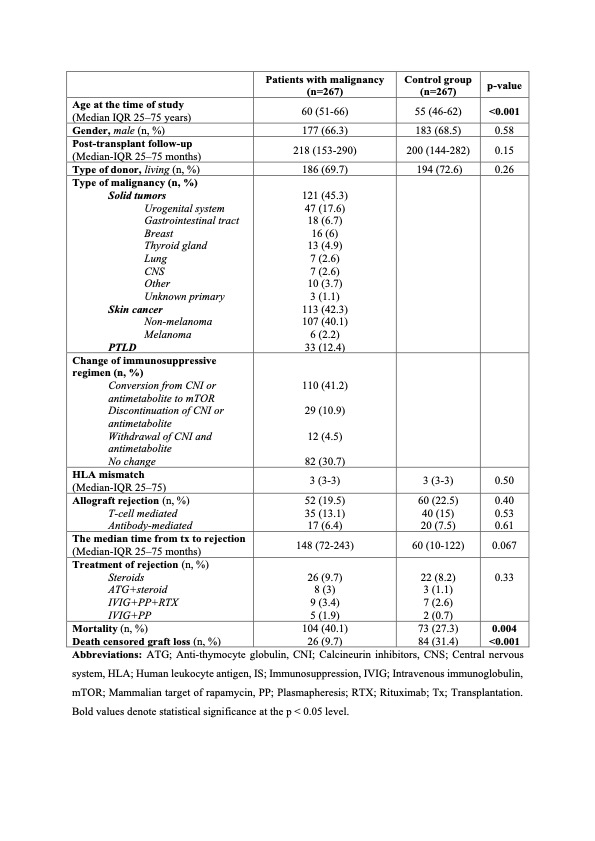
Based on Kaplan-Meier analysis, the patient group exhibited markedly lower allograft rejection rates than the control group (52 in the patient group, 60 in the control group, p = 0.043).
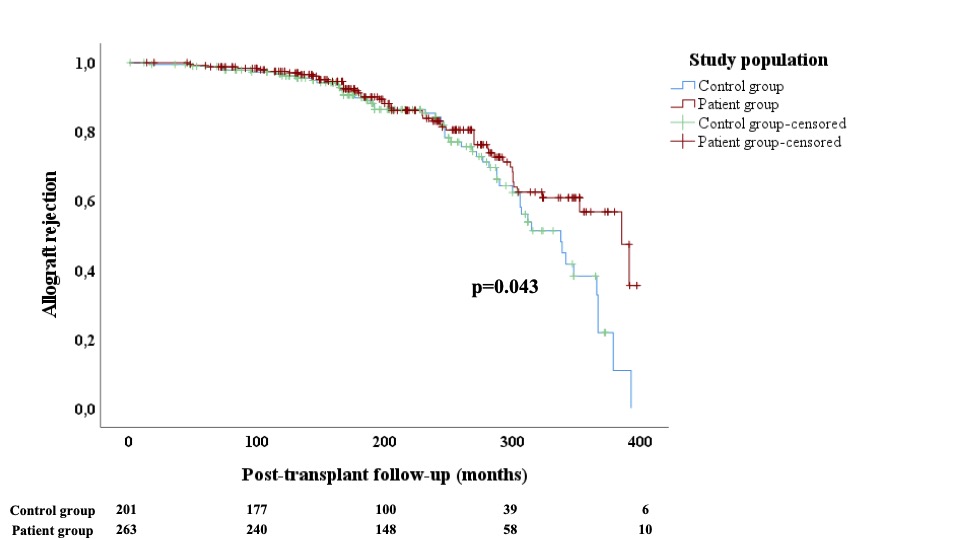
However, the observed disparity in mortality between the two groups did not achieve statistical significance (104 in the patient group, 73 in the control group, p = 0.66). Notably, individuals with malignancies displayed a notably lower rate of death-censored allograft loss in contrast to those without malignancies (26 in the patient group vs. 84 in the control group, p<0.001). The patient and control groups showed comparable survival rates at the 5th (94% vs. 94%; p=0.131), 10th year (88% vs. 91%; p=0.549), and 15th year (47% vs. 57%; p=0.618). Regarding allograft survival rates, the patient group demonstrated significantly higher rates compared to the control group in the 5th year (99% vs. 96%; p=0.565), the 10th year (98% vs. 91%; p=0.042), and the 15th year (76% vs. 38%; p<0.001). In the multivariable regression analysis, conversion from calcineurin inhibitors or antimetabolite to mTOR inhibitors reduced the risk of allograft rejection by 57% (OR: 0.426 [95% CI: 0.204-0.887], p=0.023).
Conclusion: The malignancy in kidney transplant recipients does not appear to increase the risk of allograft rejection. Adjusting immunosuppressive therapy by conversion to mTOR inhibitors after malignancy diagnosis may effectively reduce the occurrence of allograft rejection in this patient population if contraindications are considered carefully.
[1] kidney transplantation
[2] allograft rejections
[3] malignancy
