Impact of CYP3A5 gene polymorphism on tacrolimus pharmacokinetics in kidney transplant patients in Kazakh population
Islam Madadov1, Bolatbek Baimakhanov1, Belgibayev Yernur1, Elshad Nabiyev1, Nursultan Saduakas1, Berik Rgebayev1, Farida Bolysbayeva1, Aruzhan Bayzhan1, Altynai Kali1.
1Kidney transplantation, urology and nephrology, National Scientific Center of Surgery, Almaty, Kazakhstan
Introduction: The calcineurin inhibitors tacrolimus is catalyzed by cytochrome P450 CYP3A enzymes.
The wild-type CYP3A5 *1 allele is associated with greater production of functional CYP3A5 enzyme, thus leading to higher drug-metabolizing activity by CYP3A overall. The CYP3A45*1/*1 genotype increases tacrolimus clearance by 2-fold, while the heterozygous CYP3A5*1/*3 genotype results in approximately 1.7-fold greater clearance compared to the CYP3A5*3/*3 population CYP3A5 *3/*3 has 48% lower oral clearance compared to CYP3A5 expressers.
Material and Methods: We retrospectively studied 80 kidney transplant recipients. Of them – 32 were female and 48 male patients. Mean age 36±12 years old. All patients were selected from Kazakh population and were investigated for CYP3A5 genetic polymorphism (single-nucleotide polymorphism, rs776746, also known as 6986A>G). Patients underwent related living donor kidney transplantation. There were no substantial differences in surgical technique or warm/cold ischemic times. Graft function was immediate in all cases.
Results: According to the results in our study 61.25% (n=49) of patients were homozygotes, CYP3A5*3*3 carriers (non-expressers) and 38.75% (n=31) were heterozygotes, CYP3A5*1*3 carriers (with one expressor allele). Patients were arranged by sex/type of polymorphism by Fisher’s test. There were no significant differences in sex/CYP3A5 genetic polymorphism in patients.
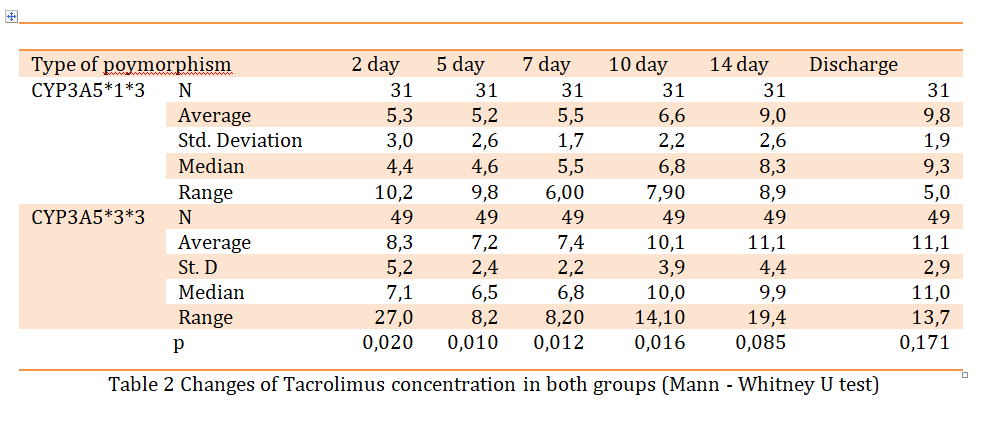
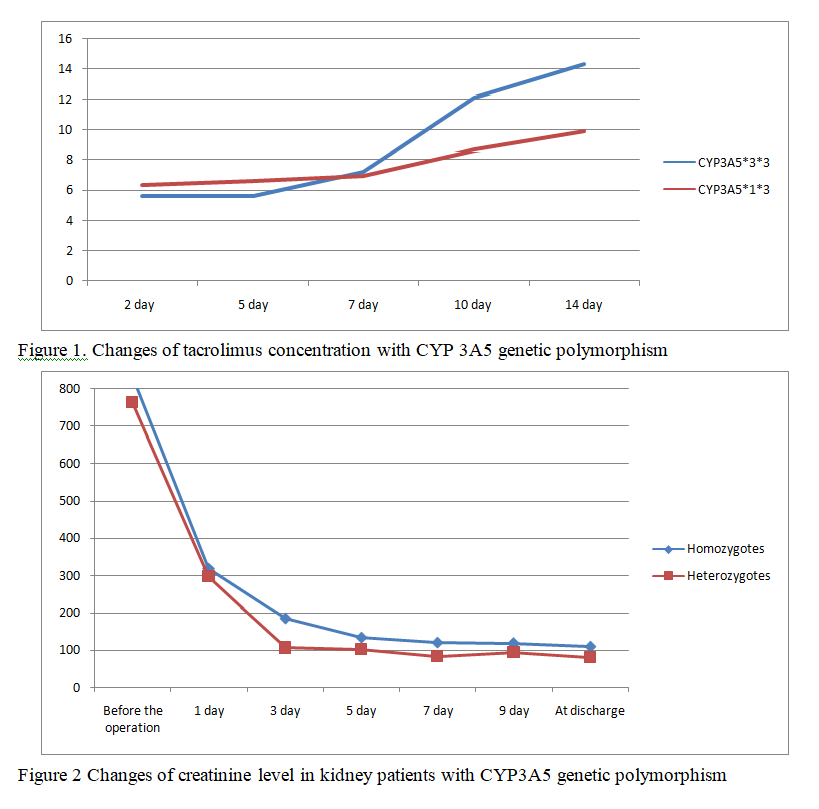
Patients were divided into 2 groups: homozygotes and heterozygotes. Тасrolimus concentration was measured on 2, 5th , 7th , 10th and 14th days after surgery and at discharge. There were significant differences in concentrations on 2nd, 5th, 7th and 10th days in both groups (p = 0.02, 0.01, 0.12 and 0.016, respectively). There were no significant statistical differences in tacrolimus concentration on 14 day after the surgery and at discharge (p = 0.085 and 0.171, respectively). In both groups tacrolimus almost reached target level at the end of 2nd week, but in heterozygotes increase was more gradual and predictable rather than in homozygotes. There were no substantial differences in graft function . Creatinine level normalized gradually in both groups and there was not significant differences in both groups at discharge (p = 0.834).
Conclusion: In Kazakh population most patients are non-expressers and this is a national characteristic. Patients reached tacrolimus trough level quickly at low doses. We expect that genotype-based dosing may be the key factor in determination of preferred doses of tacrolimus in each individual. Moreover, genotype-based patterns of dose regimen are now being investigated in order to ease the choice of suitable dose regimen. Rational immunosuppressive treatment leads to prolonged graft function and genetic factors appear to be the key factor in drug dose selection.
[1] tacrolimus, kidney transplantation, genetic polymorphism, immunosuppression.
