Laparoscopic hand-assisted donor heminephrectomy in living donor with horseshoe kidney with non-touch technique
Islam Madadov1, Aruzhan Bayzhan1, Nursultan Saduakas1, Berik Rgebayev1, Farida Bolysbayeva1, Bolatbek Baimakhanov1.
1Kidney transplantation, urology and nephrology, National Scientific Center of Surgery, Almaty, Kazakhstan
Introduction: HSK is a congenital anomaly that is characterized by the fusion of lower poles of both kidneys, with lower than usual location, just below the inferior mesenteric artery. The incidence is approximately 1 in 400-500 adults and are more frequently encountered in males (M\F ratio is 2:1) [ Kumar P, et al. 2007; Amin J. Barakat et al. 2016] . The vast majority of cases are sporadic, except for those associated with genetic syndromes [ Tischkowitz MD et al. 2003 ].
Materials and methods: 39-years old male with ESRD, for the last 2 years of haemodialysis, admitted to our center for kidney transplantation. Recipient had concurrent arterial hypertension and otherwise there were no contraindications for transplantation during preoperative evaluation. Donor was his mother 66 –years old, with arterial hypertension 1 stage (AP max 142/90 mmhg), during preoperative evaluation otherwise healthy. Due to lack of others younger related donors, we inform patients about potential risks of donation and after informed consent taken we prepared patients for surgery.
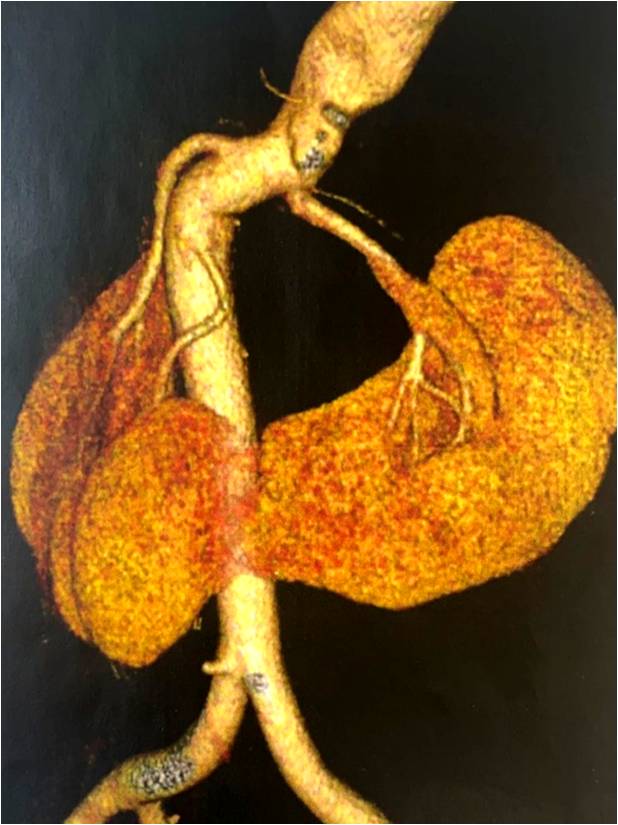
On CT scan donor had HSK, revealed first in her life, with parenchymal isthmus, 4 arteries on right half and 2 arteries on the left and the latter had retrocaval position, with aortocaval transposition that is sometimes seen in patients with horseshoe kidneys.
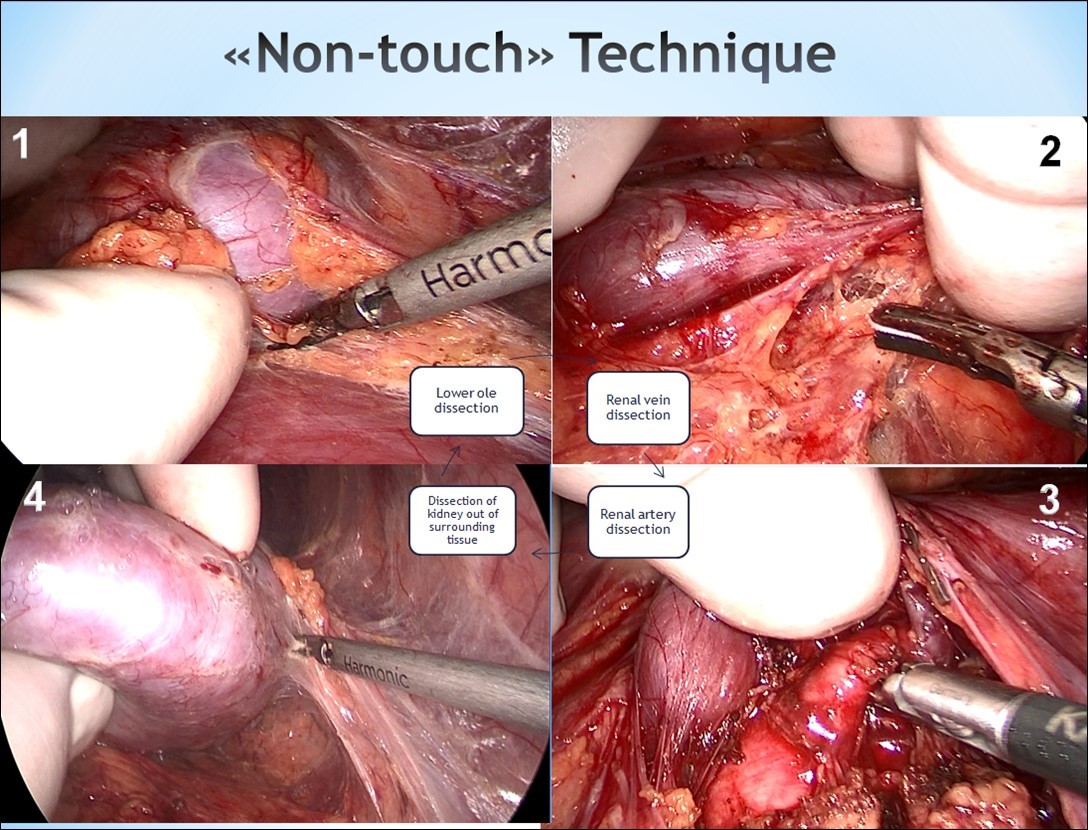
Patient underwent laparoscopic hand-assisted donor heminephrectomy by “not-touch” techinque. Firstly kidney vessels were dissected after it was fully freed out of surrounding tissue. Then isthmus was sewed in the middle and tied on both sides after left half of HSK was devascularized and then the isthmus was quickly transected just above the suture line, preventing bleeding from the right half.
Results: In our center for the last 10 years we performed more than 500 laparoscopic hand-assisted donor nephrectomies. The difference between classical nephrectomy and the latter is the precise dissection of renal vessels in order to have maximal length for engraftment. Mostly access to the renal hilum lies from dissection and lifting the lower pole, that was impossible in this case. We decided to take left half as it had fewer arteries and easier to engraft.
Warm ischemic time 1 was 92 seconds. Resected isthmus was sutured on back-table by interrupted suture and haemostatic sponge. Surgery was completed otherwise uneventfully. In case of HSK it is common problem the anomaly of kidney vasculature, pelvicalyceal system, isthmus.
Conclusion: These pitfalls are not a contraindication for organ donation anymore. There are different techniques of organ procurement but in developing surgical era we must utilize minimal invasive approaches in these patients also as to affect their recovery period and return to their daily activity.
[1] kidney transplantation
[2] heminephrectomy
[3] horseshoe kidney
[4] non touch technique
