Devprakash Choudhary, India has been granted the TTS 2023 Research Grant Award
Vascular reconstruction of multiple renal arteries - A risk factor for transplant renal artery stenosis: Insight from a matched case-control study
Devprakash Choudhary1, Rajesh Vijayvergiya 2, Arun Panjathia 1, Bharat Bamaniya 1, Sai Praneeth Reddy Perugu 1, Jasmine Sethi 3, Ujjwal Gorsi 4, Sarbpreet Singh 1, Deepesh Kenwar 1, Ashish Sharma 1.
1Department of Renal Transplant Surgery , PGIMER , Chandigarh, India; 2Department of Cardiology , PGIMER , Chandigarh , India; 3Department of Nephrology , PGIMER , Chandigarh, India; 4Department of Radiology , PGIMER , Chandigarh , India
Introduction: Transplant Renal Artery Stenosis (TRAS) stands as the leading vascular complication following kidney transplantation (KT), posing a significant threat to graft longevity and elevating mortality risk post-KT. Prompt diagnosis and timely intervention can prevent irreversible allograft damage caused by TRAS. A substantial body of research has identified several risk-factors for TRAS, such as prolonged cold ischemia-time, extended-criteria donors, and delayed graft function, primarily in the context of deceased donor-KT. However, a significant gap persists in comprehending specific risk factors for TRAS and its long-term outcomes in living donor-KT. This matched case-control study, conducted at a premier national transplant center that predominantly performs living donor-KT, assesses various risk factors and long-term outcomes of clinical-TRAS (cTRAS) in kidney transplant recipients(KTRs).
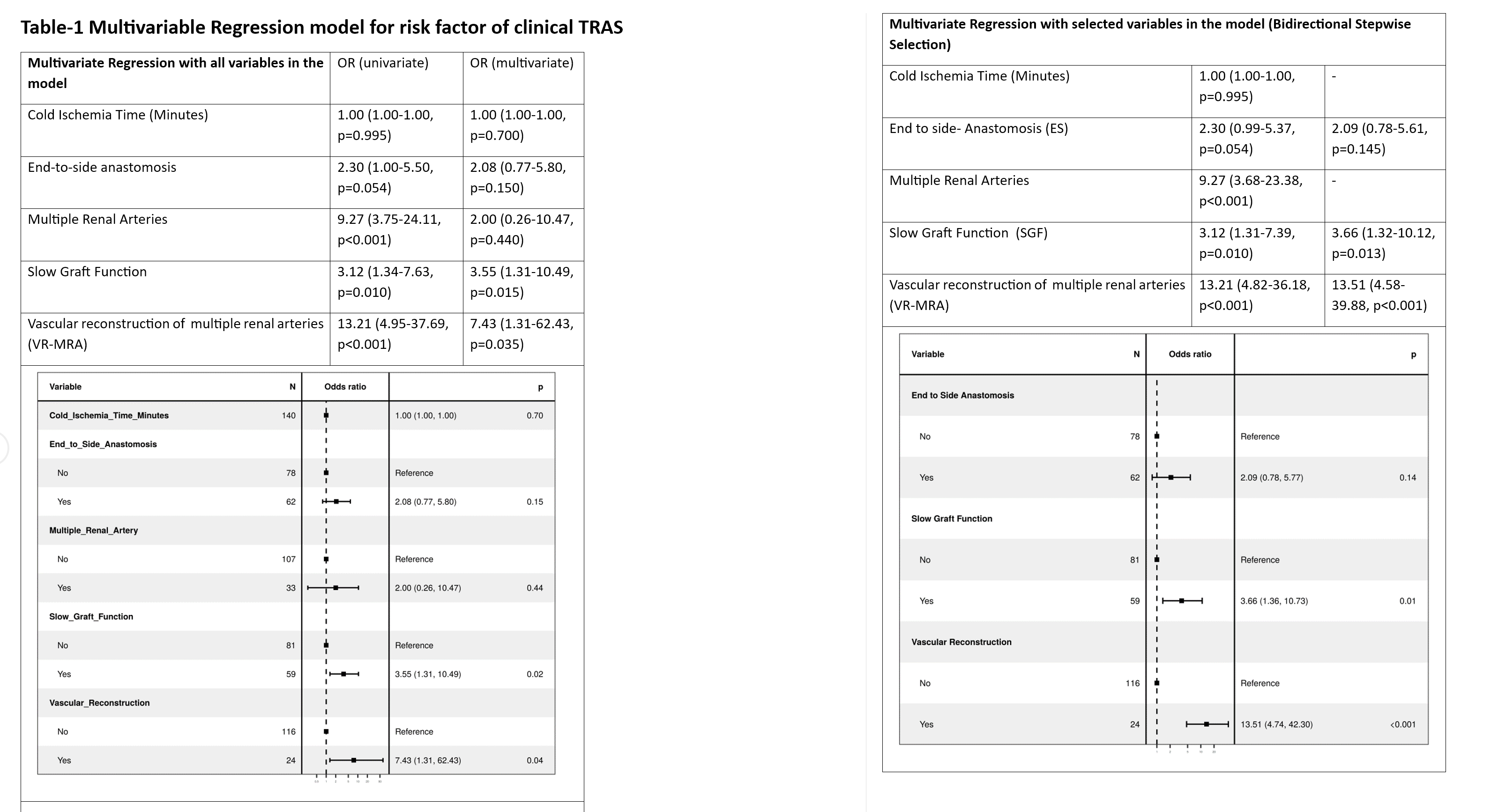
Methods: cTRAS cases diagnosed from January 2007 to December 2022 were individually matched with four control KTRs to control for various confounding factors. The study was powered to evaluate whether ex-vivo arterial vascular reconstruction of multiple renal arteries (VR-MRA) increases the risk of cTRAS by employing a dual-method analytical framework integrating multivariable regression analysis with all predictor variables and bidirectional stepwise selection to assess VR-MRA's impact on increased risk of cTRAS development.
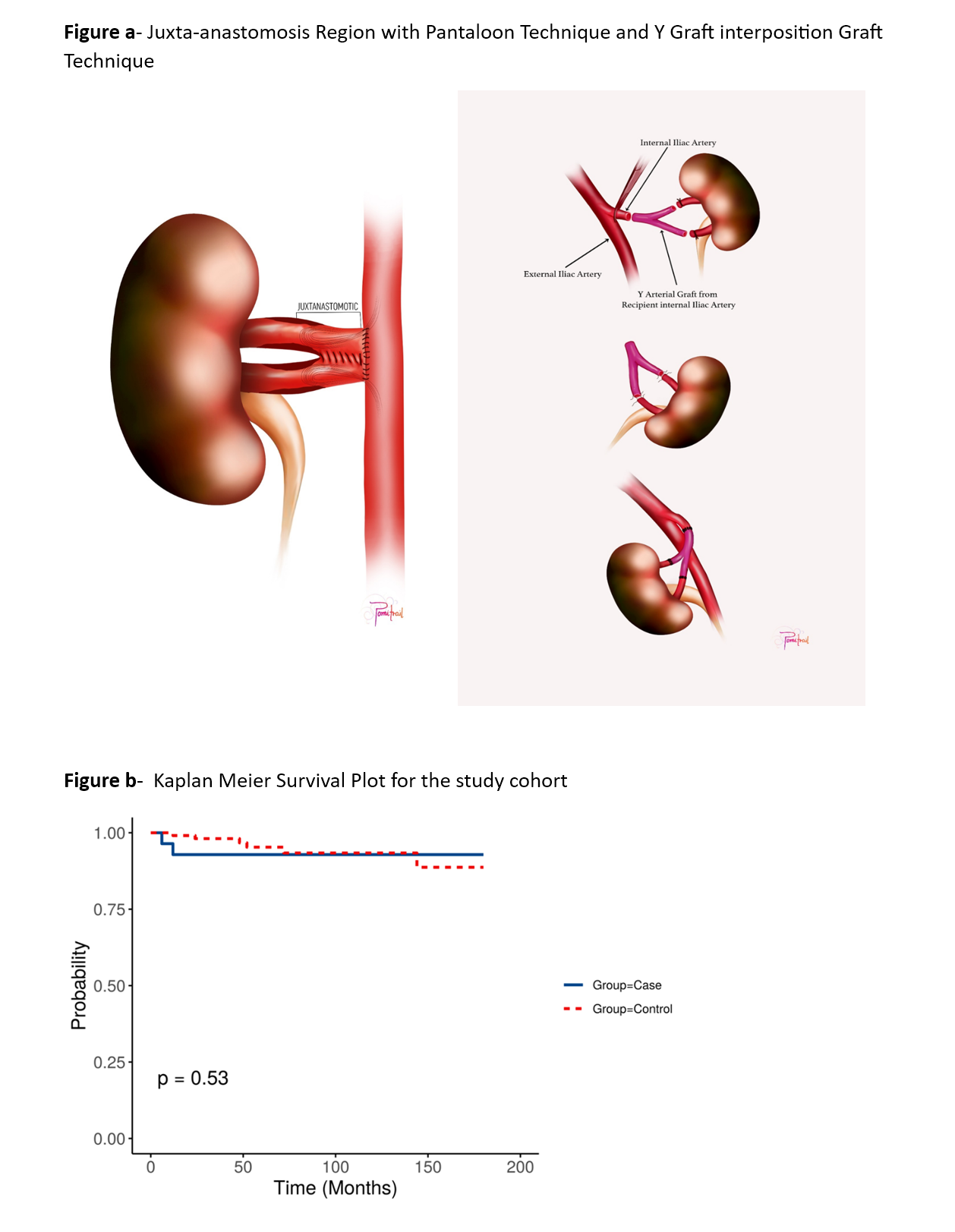
Results: Of the 2,454 KT performed during the study period, 28 KTRs (1.14%) were diagnosed with cTRAS around 3.62 ± 1.04 months post-KT, with stenosis predominantly in the juxta-anastomotic region. The majority of cTRAS cases (92.86%) presented with renal allograft dysfunction, with 57.14% of them necessitated ≥2 antihypertensive medications. Mild acute tubular necrosis was the most common biopsy finding in 67.85% of cTRAS cases. Endovascular intervention as percutaneous transluminal angioplasty (PTA), accompanied by stenting, was performed in 89.28% of cases, while PTA alone was utilized in three cases. All cTRAS cases demonstrated favorable outcomes over 6-180 months of follow-up. Recurrence of cTRAS occurred in two cases, leading to a 7.14% reintervention rate. Both these cases were successfully treated with cutting balloon-angioplasty and drug-eluting stenting. A significant finding of this study is the identification of ex-vivo VR-MRA as an independent risk factor for cTRAS (P<0.001) (Figure-a, table-1). Notably, cTRAS cases and control KTRs demonstrated comparable long-term graft and patient survival rates (figure-b)
Conclusion: This largest single-center experience from Asia on clinical-TRAS underscores VR-MRA as a significant independent risk factor for cTRAS. We advocate for regular color Doppler screening during the initial six months post-KT, especially in KTRs with VR-MRA and unexplained renal allograft dysfunction, to ensure prompt detection and timely intervention.
We sincerely thank Dr. Kamal Kishore and the Transplant Coordinator team of PGIMER for their valuable insights and contributions to this work.
[1] Transplant Renal Artery Stenosis
[2] Multiple Renal Arteries
[3] Renal Allograft Dysfunction
[4] Endovascular Intervention
[5] Clinical Transplant Renal Artery Stenosis
[6] Vascular Reconstruction
[7] Living Donor Kidney Transplantation
[8] Duplex Ultrasonography Screening
[9] Renal Allograft Survival
[10] Drug-Eluting Stents
