Glissonean approach and parenchymal dissection with water jet scalpel for liver transplantation living donor
Yasuhiro Fujimoto1, Nobuhiko Kurata1, Tomoki Ebata2, Yasuhiro Ogura1.
1Transplantation Surgery, Nagoya University Hospital, Nagoya, Japan; 2Department of Surgery, Nagoya University Graduate School of Medicine, Nagoya, Japan
Introduction: When performing a donor hepatectomy procedure, there are several key points to consider, as appropriate margins for both blood vessels and bile ducts are important for anastomosis in the recipient, as well as stump closure in the donor. Moreover, blood supply around the bile ducts should be secured to avoid anastomotic stricture in the recipient. When performing a hepatic parenchymal resection, bleeding should be limited as much as possible and parenchymal cauterization for hemostasis must be minimized to avoid damage to liver tissue. For these purposes, introduced here is a Glissonean approach for dissection around the hepatic hilum with use of an ERBEJET® 2 water jet scalpel for parenchymal dissection.
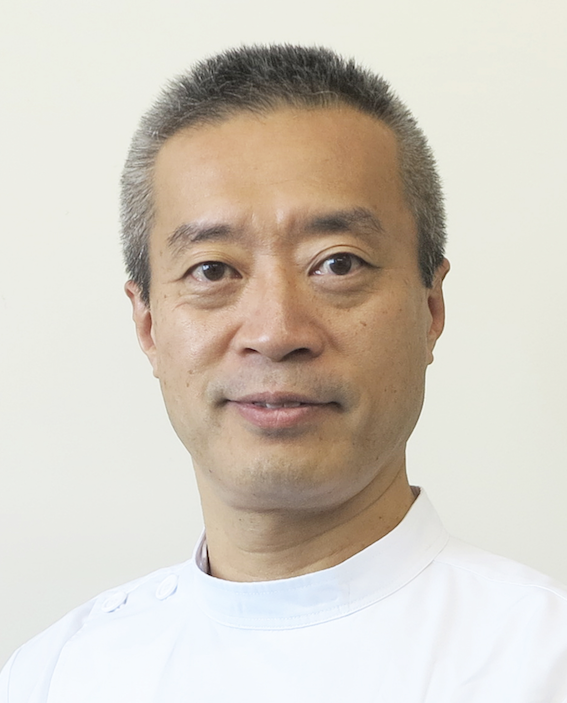
Methods: With focus on the factors noted above, successful hepatic parenchymal resection procedures were performed for two right-lobe donors, both female, 43 and 42 years old, respectively. Following are details regarding the techniques used. (1) A laparotomy is performed via an inverted-T incision, (2) then the right lobe is mobilized to the inferior vena cava. (3) Next, a whole layer cholecystectomy is performed to clarify important details for the approach to the right Glissonean pedicle, which is encircled with rubber tape. (4) The demarcation line on the liver surface is then delineated by temporary clamping of the right pedicle to provide a line for dissection. (5) Using the tape around the Glissonean pedicle as a guide, a Penrose drain is passed between the pedicle and hepatic parenchyma.
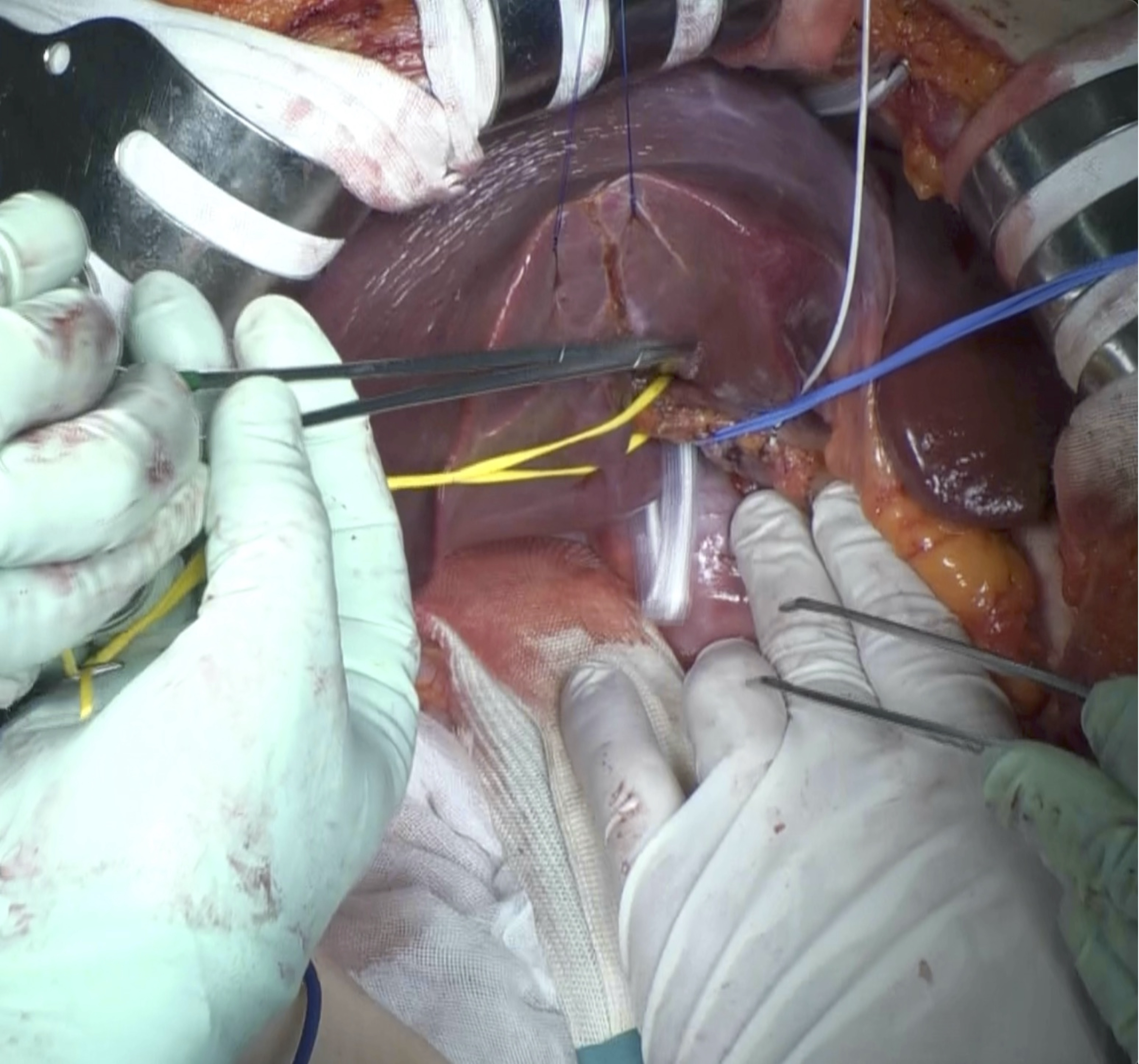
(6) The hepatic parenchyma is then dissected with water jet scalpel as a dissector, bipolar cautery to cauterize small vessels and scissors to cut cauterized structure.
Dissection plain is clarified with the middle hepatic vein used as an indicator in the liver, and the Penrose drain to indicate the posterior surface as well as the cutting line to follow. At this stage, the grafted liver is connected to the remaining liver only by the right Glissonean pedicle and right hepatic vein. (7) The right hepatic artery and right portal vein are then subtracted from the pedicle, leaving only the right bile duct remaining taped. Cholangiography is used determine the root of the right hepatic duct then bile duct dissection is performed. (8) Each vessel is dissected, then the grafted liver portion is removed from the donor. (9) Finally, the ducts are closed and hemostasis is confirmed, after which the wound is closed with no drain.
Results: Operation time for the present cases was 394 and 413 minutes, respectively, while blood loss was 200 and 354 cc, respectively. No complications were observed in the donors or recipients.
Conclusion: Use of the techniques introduced here ensures preservation of the periductal blood supply and facilitates reduction of bleeding during a hepatic parenchymal resection procedure.
[1] living donor liver transplantation
[2] hepatectomy
[3] Glissonean approach
[4] water jet scalpel
