Is not treating ≤3000 IU /ml of Cytomegalovirus viremia safe in living donor R+D+ renal transplant recipients?
Sunil Kumar Dodani1, Asma Nasim1.
1Infectious Disease, Sindh Institute of Urology and Transplantation, Karachi, Pakistan
Introduction: Cytomegalovirus (CMV) infection after renal transplantation can cause graft dysfunction with morbidity and mortality. Our center is an exclusive living donor program with 99% R+D+. Due to non-availability and cost of oral valgancylovir, we opt for event driven CMV treatment. Our protocol is to treat all CMV infection with viral load of >3000 IU/ml. However some patients did receive treatment with lower viral loads. The aim of this study is to assess the outcome of not treating patients with viral load ≤3000 copies/ml among living donor D+R+ renal transplant recipients.
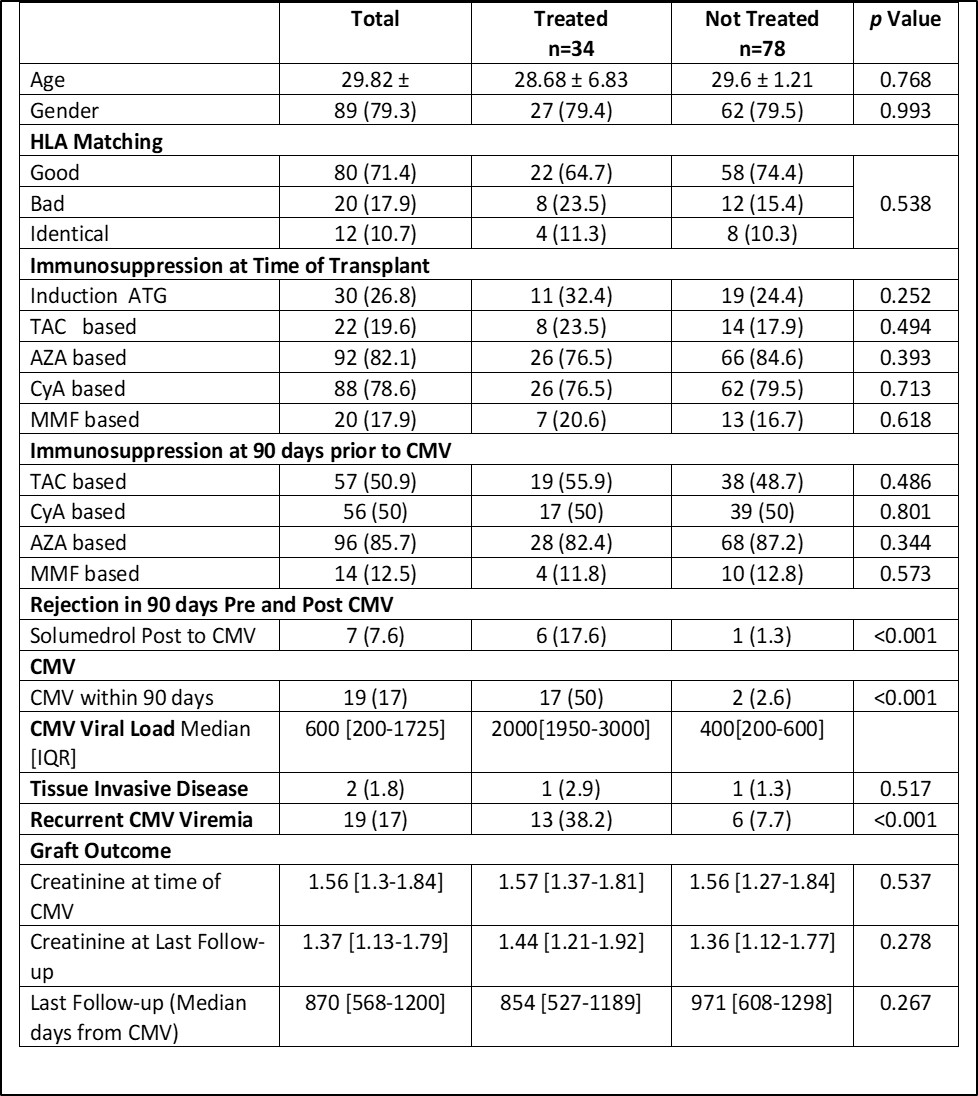
Methods: The files of renal transplant recipients who receive graft from January 2018 to December 2020 and who have CMV viral load of ≤ 3000 are included. The first CMV episode is taken. Patient are divided into those who are treated and those who are not. Demographics, HLA match, time since transplant, immunosuppression at the time of transplant and 90 days before CMV episode, rejection 90 days before and after CMV episode, tissue invasive disease, recurrent CMV and serum creatinine at the last follow up (4 years post-transplant) are compared.
Results: A total of 112 had viral load of ≤3000 IU/ml. Out of these 78 (69.3%) are not treated. Age, gender, HLA match and immunosuppression are comparable. Median viral load was 600 IU/ml. Significantly more patients were treated within 90 days post-transplant. There is no difference in the development of tissue invasive disease. Recurrent CMV is seen significantly more in treatment group. Moreover significantly more patients develop rejection in treatment group and received solumederal. There is no difference in graft outcome at the last follow up between treatment and no treatment group. Table 1 shows the outcome in more detail.
Conclusion: Viral load ≤3000 can safely be not treated in D+R+ living donor renal transplant recipients.
[1] Cytomegalovirus
[2] viremia
[3] Renal Transplant
