Pediatric kidney transplantation in Dubai. Outcomes and challenges
Marwa Mohamed1,2,3, Abdalazeez Alghraizat 1, Hazem Awad1, Haneen Yamin1, Shameer Habeeb1, Eva Simkova1, Entesar Alhammadi1,3, Loai Eid1,3, Waldo Concepcion1,3,4, Martin Bitzan1,3.
1Kidney Center of Excellence, Al Jalila Children's Hospital, Dubai, United Arab Emirates; 2Surgical Oncology Resaerch, Massachusetts General Hospital, Boston, MA, United States; 3Transplant Surgery, Al Jalila Children's Hospital, Dubai, United Arab Emirates; 4Mohammed Bin Rashid University of Medicine and Health Sciences , Dubai, United Arab Emirates
Introduction The UAE is a young, rapidly developing country with a unique, ethnically and culturally diverse population. The spectrum of pediatric CKD has not been systematically studied, and the kidney transplant (KT) infrastructure is still evolving.
Aims of the study: to evaluate KT outcomes at a pediatric tertiary care hospital. Outcomes of interest were ESKD causes, rates of living related (LRD) and deceased donor (DD) kidney utilization, age at KT, time on dialysis, and patient and graft survival.
Method Retrospective single-center cohort study encompassing all children transplanted at the Al Jalila Children’s Hospital. Standard immunosuppression consisted of induction with a lymphocyte depleting antibody (Grafalon) or basiliximab, glucocorticoids, mycophenolate and tacrolimus. Data analysis is descriptive. Continuous variables are shown as median and range. Categorical variables are presented numerically or as percent.
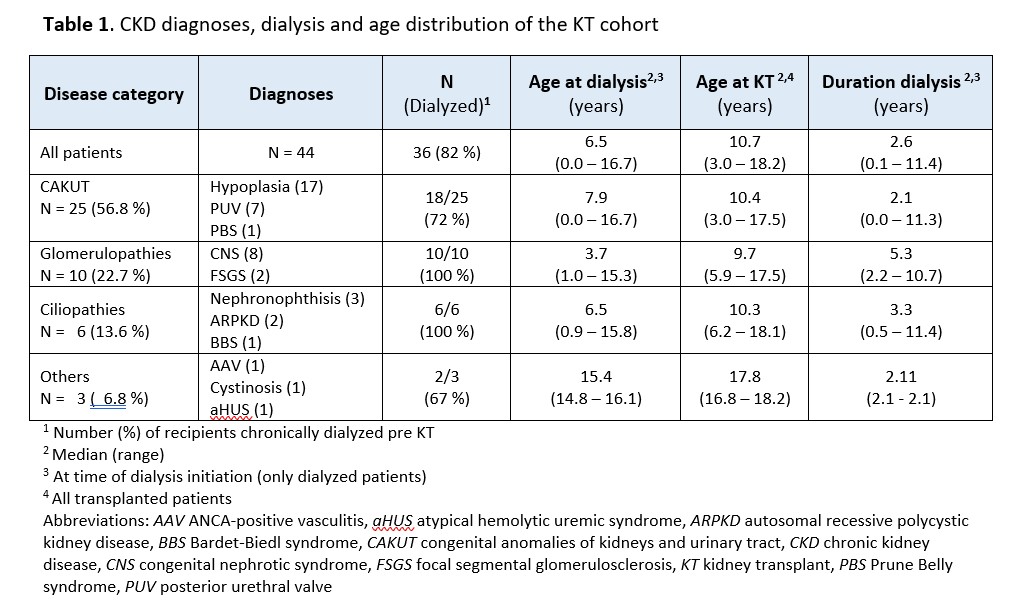
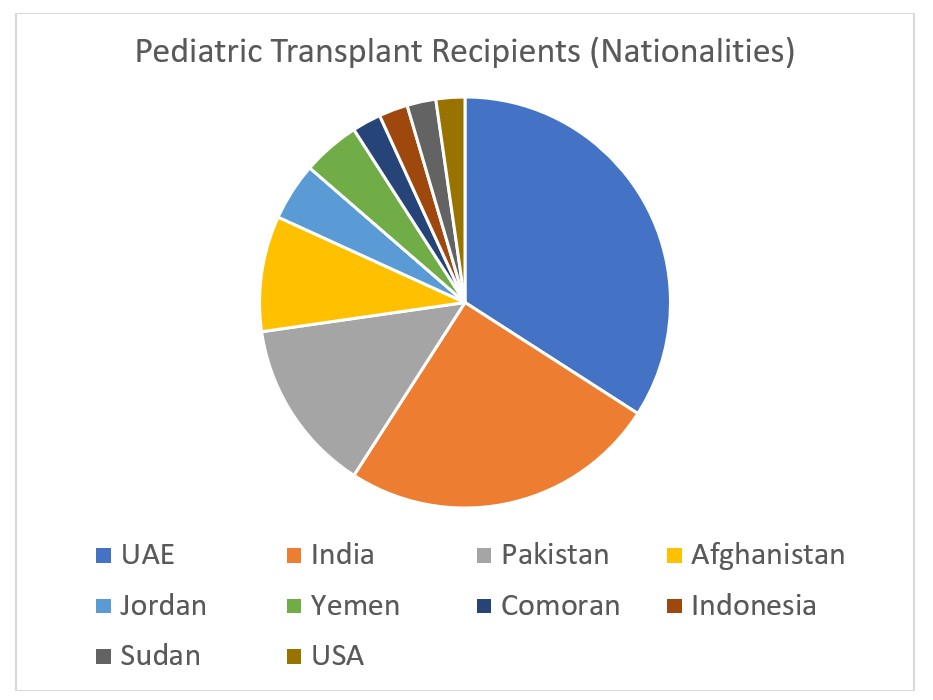
Results Since the inception of the program in 10/2018, 44 children were transplanted at our centre. Congenital anomalies of the kidneys and urinary tract (CAKUT) contributed 57% of CKD5 patients, followed by glomerulopathies (18%; Table 1). A genetic cause was identified in 41% of patients. Ethnic diversity and geographic origin of the transplanted patients mirror the population mix in the UAE (Fig 1). 82% of children underwent chronic hemo- or peritoneal dialysis prior to KT. Age at dialysis initiation was 6.7 (0.0–16.7) and at KT 10.7 (3.0-18.2) years (Table 1). Spent dialysis time was 2.6 (0.1-11.4 ) years, wait time after listing 5.3 (0.07-32.7) months. Patient and graft survival were 100 and 95.5%, respectively. 2/44 grafts were lost due to early technical complications. Biopsy-proven graft rejection occurred in 10/44 patients (23%). Isolated T cell- (TCMR) and antibody-mediated rejection (ABMR) was found in 4 patients each, and mixed TCMR and ABMR in 2/10 patients. One patient developed histologically evident polyomavirus BK nephropathy (0.0125 cases per patient year). No symptomatic EBV or CMV infections or post-transplant lymphoproliferative disease (PTLD) was observed.
Conclusion The approximate incidence of CDK5 is 11 per million pediatric population (pmpp), similar to USRDS data. Salient features of our cohort are high proportions of CAKUT (57%) and congenital nephrotic syndromes (18%), both substantially exceeding USRDS figures. A genetic cause of CKD was found in 41%. CAKUT patients had the highest rates of preemptive KT (28%). The DD to LRD transplant ratio was 3.3/1. One- and 2-year graft and patient survival compare favorably with international registries. Prevalent dialysis rates have not yet diminished despite an established national pediatric priority allocation policy. Current challenges are (1) to increase living and deceased organ donations and transplantation rates, and (2) secure sustainable funding for chronic dialysis, transplantation and post-transplant care for non-national residents.
[1] Kidney transplant
[2] Endstage kidney disease
[3] CAKUT
[4] anti-T lymphocyte globulin
[5] Epidemiology
[6] Graft rejection
[7] Immunosuppression
[8] Allograft survival
[9] Pediatrics
[10] Pediatric nephrology
