Current allocation policies disadvantage young adults waitlisted after 18 years old for kidney transplantation
Justin Steggerda1,3, Steven A Wisel1,3, Dechu Puliyanda2,3, Helen Pizzo2,3, Jonathan Garrison3, Irene K Kim1,3.
1Transplant Surgery, Cedars-Sinai Medical Center, Los Angeles, CA, United States; 2Pediatric Nephrology, Cedars-Sinai Medical Center, Los Angeles, CA, United States; 3Comprehensive Transplant Center, Cedars-Sinai Medical Center, Los Angeles, CA, United States
Introduction: Current kidney transplant (KT) policy in the United States (US) offers pediatric candidates waitlisted before turning 18 years old (yo) benefits in waiting time and organ allocation, regardless of clinical condition at time of waitlisting. This study investigates the impact of such allocation policies on candidates who initiate dialysis prior to 18yo but register as adults (≥18yo).
Methods: The OPTN STAR database was used to evaluate outcomes for patients waitlisted as 11-25 year-olds between 2001-2022 in the US. Multiple registrations and multivisceral listings were removed. Patient cohorts were defined as: Peds if <18yo, Adult if ≥18yo; and NYOD- not yet on dialysis or OD- on dialysis, at time of listing with adult groups distinguished by age at dialysis initiation. Outcomes of listing, transplant characteristics, and graft survival were assessed across groups. P-values <0.01 were considered significant.
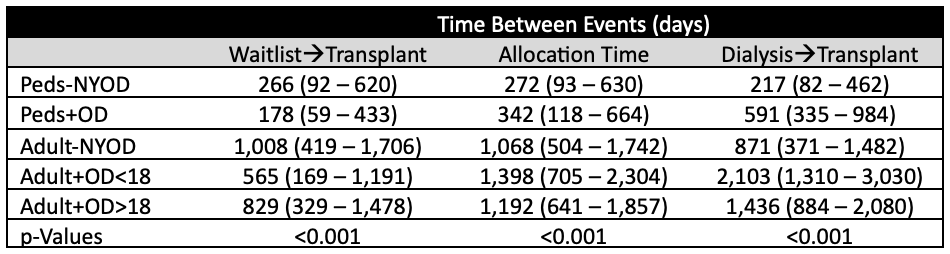
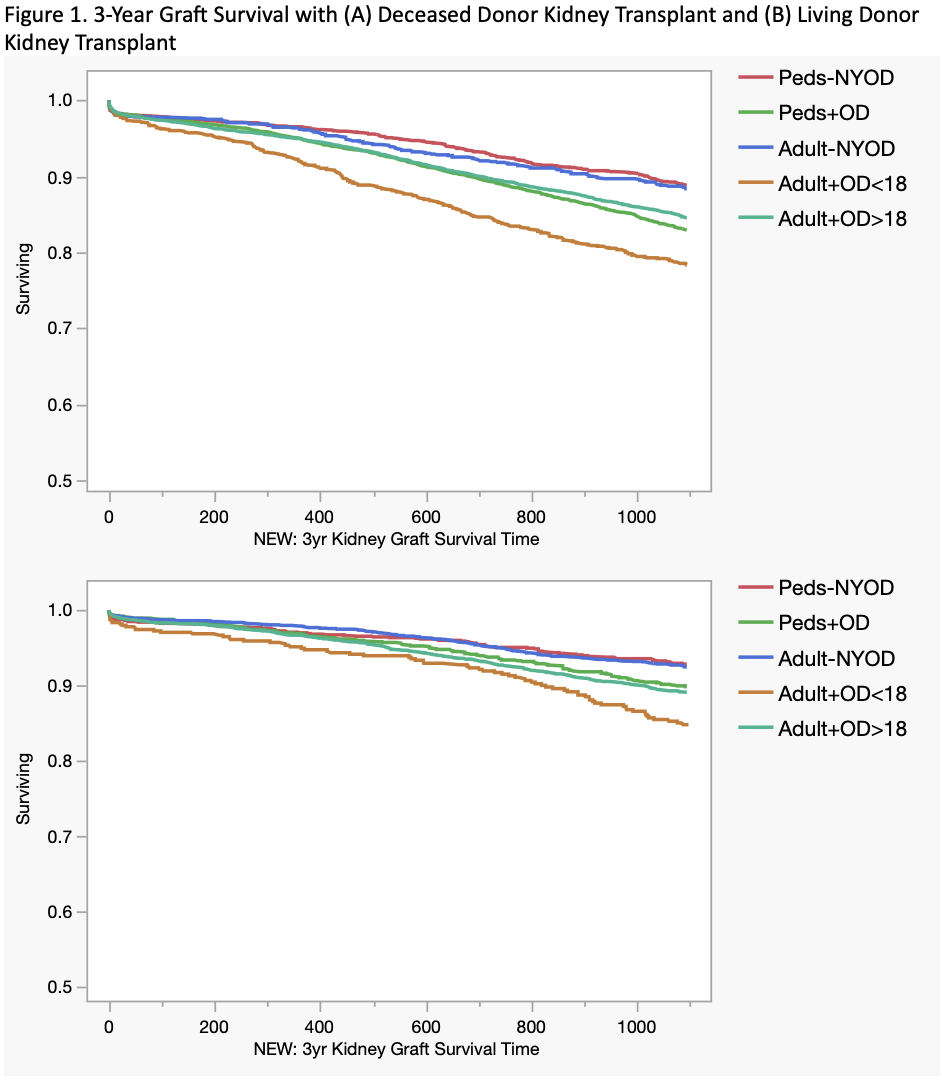
Results: Of 35,764 registrations identified, 4,764 (13.3%) were Peds/NYOD, 7,169 (20.0%) were Peds+OD, 5,581 (15.6%) were Adult/NYOD, 2,965 (8.3%) were Adult+OD<18, and 15,284 (42.7%) were Adult+OD≥18. Adult+OD<18 had highest proportions of Black (32.3%), Hispanic (28.2%), and prior KT (17.5%) candidates. Of all candidates, 10,252 (28.7%) received a living donor (LD) KT, 16,228 (45.4%) received a deceased donor (DD) KT, and 9,284 (26.0%) were not transplanted. Adult+OD<18 accounted for the most non-transplanted patients (33.5%), with the highest rates of death (23.0%) and worsening condition to preclude KT (7.9%). Amongst DDKT recipients, Adult+OD<18 had the longest allocation time and spent the longest time on dialysis (Table 1, p<0.001). Adult+OD<18 recipients had worst 3-year graft survival (figure 1) and compared to Peds-NYOD, Adult+OD<18 had greatest risk of 3-year graft loss on multivariable analysis for both DDKT (hazard ratio 1.50, 95% confidence interval 1.18-1.89, p<0.001) and DDKT (HR 1.88, 95% CI 1.25-2.81).
Conclusions: In the United States, current pediatric waitlisting policies disadvantage Adult+OD<18 candidates which initiate dialysis as pediatric patients but are waitlisted as adults, leading to the highest rates of non-transplant, longest time on dialysis, and worst graft survival for both LD and DDKT. These results may inform policy development globally and demand re-examination of these policies in the US.
[1] Waitlist
[2] Pediatric Advantage
[3] Allocation Policy
[4] Waiting Time
[5] Graft Survival
