Comparison of survival advantage of simultaneous kidney-pancreas vs kidney transplant in patients with diabetes who received mate kidneys
Pooja Budhiraja1, Jesse Schold2, Rocio Lopez Moscoso2, Susana Arrigain2, Bruce Kaplan2.
1Transplant, Mayo Clinic, Phoenix, AZ, United States; 2Transplant, University of Colorado, Aurora, CO, United States
Background: Simultaneous Pancreas-Kidney Transplantation (SPKT) is believed to offer survival benefits over Deceased Donor Kidney Transplant (DDKT) because of superior donor kidney quality. However, the implications of added surgical and immunological risks from pancreas transplantation remain unclear. This study evaluates SPKT vs. DDKT outcomes in diabetic recipients receiving matched-quality mate kidneys.
Method: We conducted a retrospective analysis using the Scientific Registry of Transplant Recipients data (2006 - 2023), analyzing patient and kidney graft survival through Cox models, adjusted for donor-recipient pairing and recipient characteristics. Age-stratified effects on survival benefits were examined, calculating life-year gains as the difference in restricted mean survival time between groups.
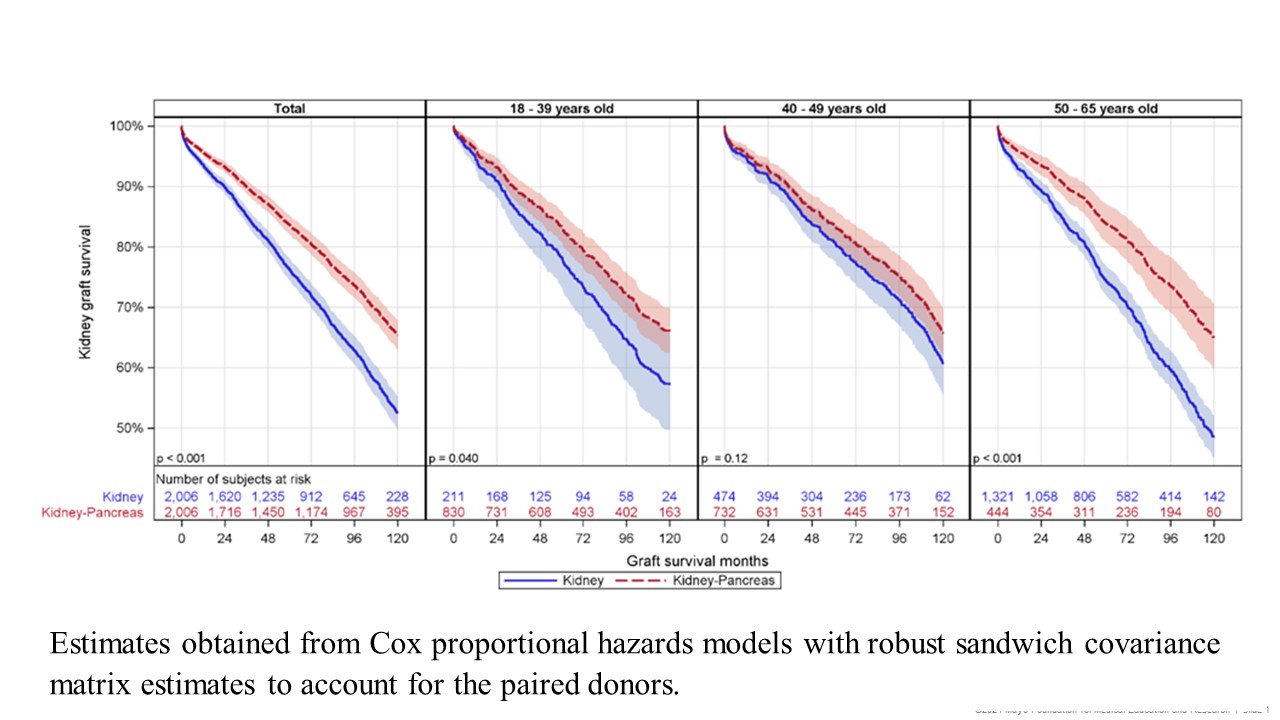
Results: The study included 4,012 recipients from 2,006 kidney pairs. SPKT recipients were younger (42 vs. 54 years for DDKT), more males, non-Hispanic White, privately insured, with lower BMI, type I diabetes, and shorter dialysis and waitlist durations. SPKT recipients had higher 5 and 10-year patients (90% and 75%) and graft (84% and 65%) survival rates than DDKT recipients (82% and 59% for patients, 76% and 52% for grafts).
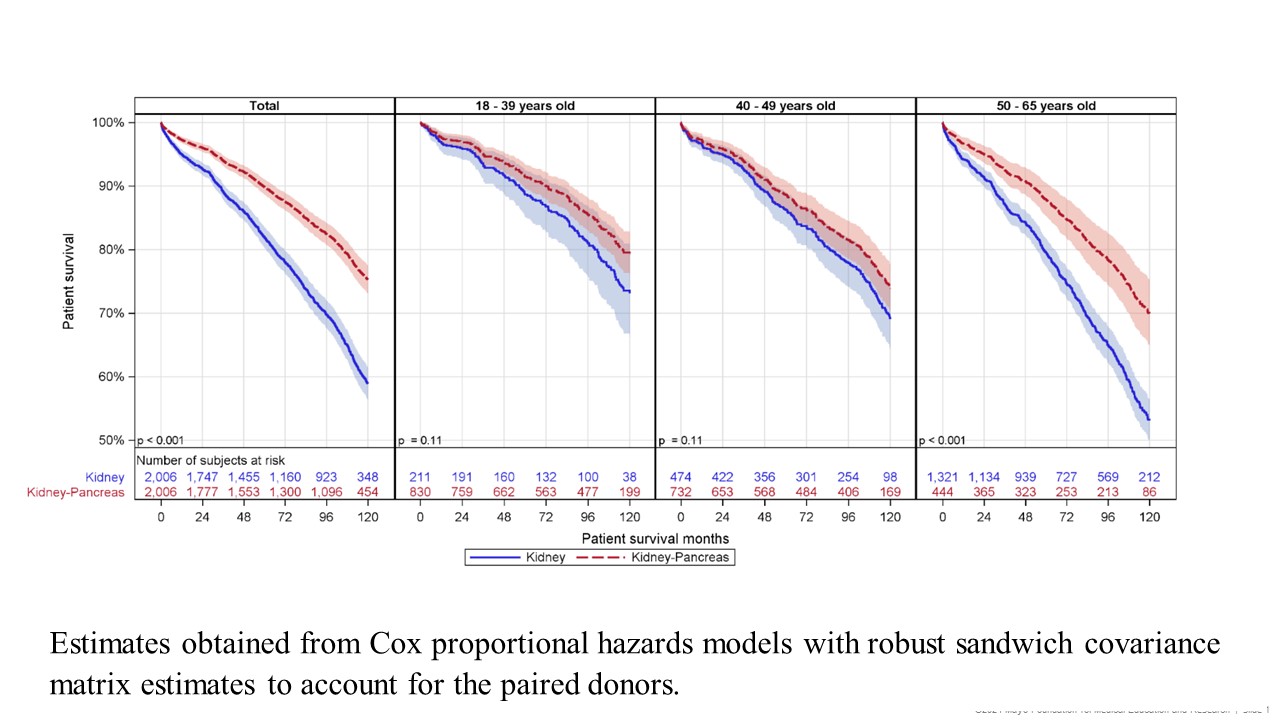
In adjusted analyses, DDKT recipients had a 28% higher 10-year mortality risk than SPKT (AHR=1.28, 95% CI: 1.07, 1.54), significantly higher in those 50-65 years (AHR=1.74, 95% CI: 1.33, 2.29) but similar in younger groups (18-39 years: AHR=1.00, 95% CI: 0.60, 1.68; 40-49 years: AHR=0.82, 95% CI: 0.59, 1.14).
DDKT's 10-year graft failure risk was 20% higher (AHR=1.20, 95% CI: 1.01, 1.42), especially at 50-65 years (AHR=1.62, 95% CI: 1.26, 2.09). SPKT provided a 14- and 13-month survival benefit for patients and grafts, respectively, in the 50-65 age range, possibly due to a healthier selection of SPKT recipients.
Conclusion: Despite matching kidney quality and higher surgical and immunological risk with simultaneous pancreas transplants, SPKT recipients demonstrate a survival advantage. These findings emphasize the importance of considering SPKT in patient counseling and organ allocation decisions.
The data reported here have been supplied by the Hennepin Healthcare Research Institute as the contractor for the SRTR. The interpretation and reporting of these data are the responsibility of the author(s) and should not be seen as an official policy or interpretation by the SRTR or the U.S. Government.
[1] pancreas, diabetes, kidney transplant, survival
