Sanjay D Dutta, Australia has been granted the TTS-TSANZ Basic and Translational Mentee-Mentor Award

Sanjay Dutta is a current Cardiothoracic and Transplant Surgery Registrar at St Vincent's Hospital Sydney.
He is also currently completing his PhD at the Victor Chang Cardiac Research Institute and The University of New South Wales under the supervision of Professor Peter Macdonald and Professor Chris Hayward, exploring methods to improve donor heart organ preservation through the use of a novel peptide derived from the venom of the Australian funnel-web spider.
Sanjay is supported by an Australian National Health and Medical Research Council (NHMRC) Dora Lush Basic Science Postgraduate Scholarship.
Improved recovery of rat hearts after prolonged cold storage by acid sensing ion channel (ASIC) inhibitor Hi1a varies with preservation solution
Sanjay Dutta1,2,3, Jeanette E Villanueva1,2, Ling Gao1, Aoife Doyle1, Nathan Palpant4,5, Glenn King4,5, Peter S Macdonald1,2,3,4.
1Cardiac Transplantation Laboratory, Victor Chang Cardiac Research Institute, Sydney, Australia; 2St Vincent’s Clinical School, The University of New South Wales, Sydney, Australia; 3Department of Heart and Lung Transplantation, St Vincent’s Hospital, Sydnet, Australia; 4Infensa Bioscience Pty Ltd, Brisbane, Australia; 5Institute for Molecular Bioscience, The University of Queensland, Brisbane, Australia
Introduction: Most heart transplantations rely on cardioplegia solution and cold static storage (CSS) for organ preservation, however long ischaemic times result in poor outcomes. Many different cardioplegia solutions are used clinically worldwide, with no evidence of superiority of one over others. Supplementation of cardioplegia solutions can improve post-transplant organ function and Hi1a, an ASIC1a inhibitor derived from funnel web spider venom, has shown promise to reduce the degree of ischaemia-reperfusion injury. We investigated the impact of supplementation of cardioplegia with Hi1a on cardiac function following CSS.
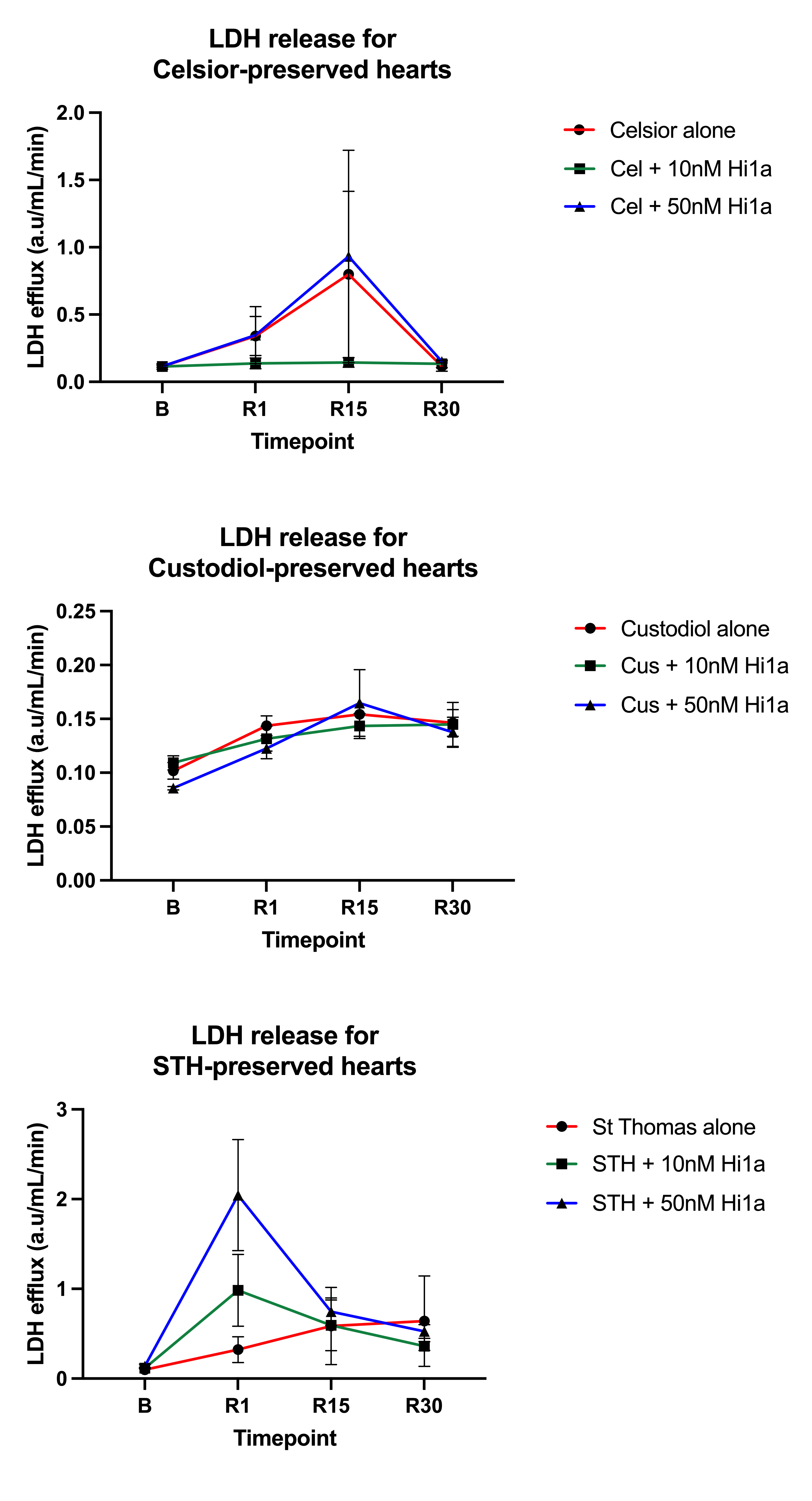
Methods: Hearts were isolated from male Wistar rats (350-570g, n = 5-8/group), perfused ex-vivo with Krebs-Henseleit buffer at 37°C, and baseline haemodynamic measurements of aortic flow (AF) were obtained. Hearts were arrested with modified St Thomas (STH), Celsior (Cel) or Custodiol (Cus) cardioplegia either alone, supplemented with 10nM Hi1a or 50nM Hi1a. Following 6-hour CSS (4°C), hearts were re-perfused ex-vivo. Haemodynamic measurements were obtained, and recovery expressed as percentage of pre-storage baseline (mean ± SEM). Coronary effluent was collected at baseline (B) prior to arrest, and at three timepoints (1 minute, 15 minutes, 30 minutes) during reperfusion (R), and assessed for lactate dehydrogenase (LDH) release as a marker of myocardial necrosis.
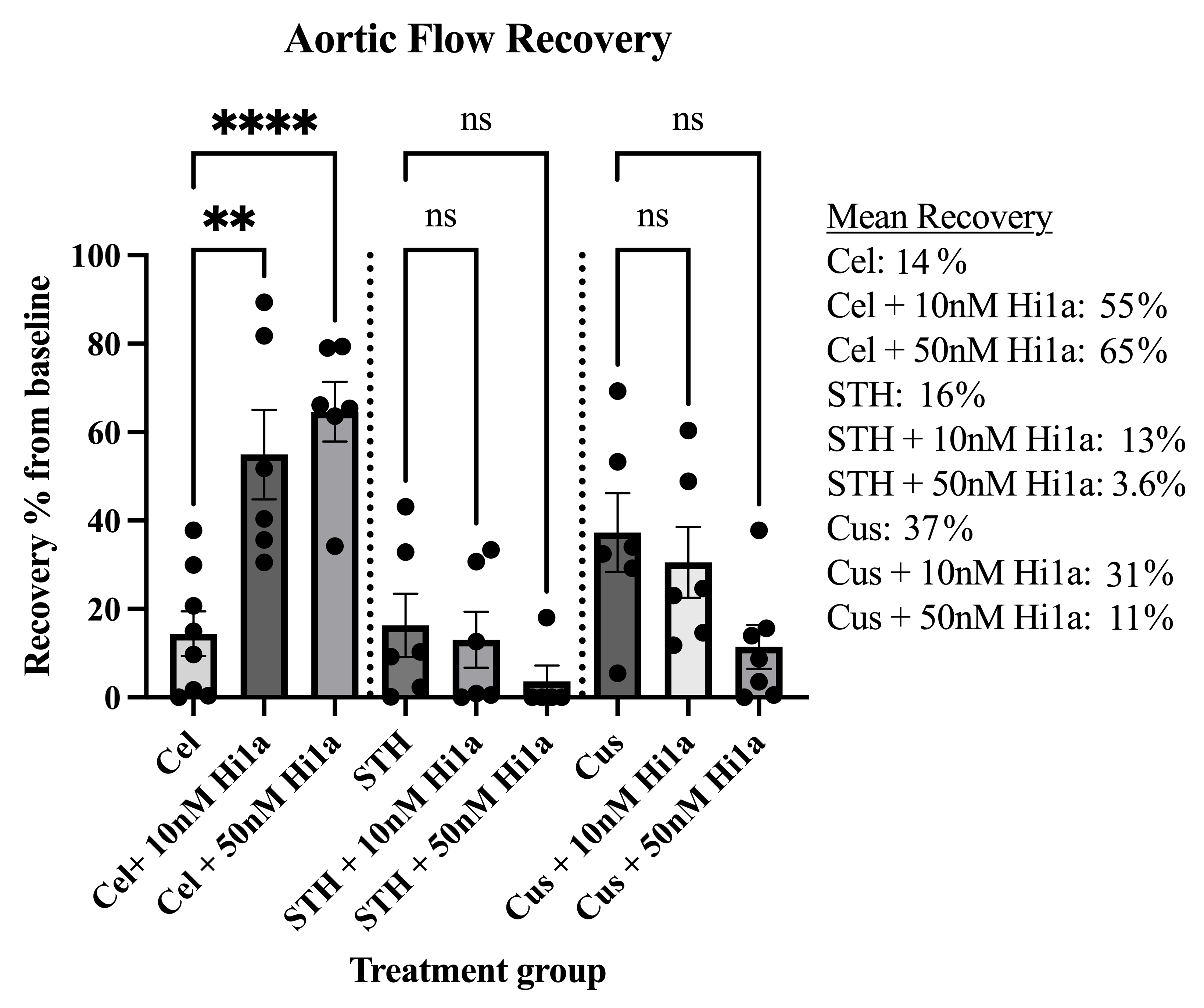
Results: As shown in Figure 1, compared to unsupplemented Celsior (AF 14±5.0%) hearts stored in Celsior supplemented with either 10nM Hi1a (AF 55±10%, P = 0.026) or 50nM Hi1a (65±6.7%, P < 0.001) showed significantly improved recovery in a dose-dependent manner. Hearts stored in Custodiol trended towards worse recovery when supplemented with both 10nM and 50nM Hi1a. Hearts stored in STH had poor recovery of AF, with and without supplementation. Coronary effluent from hearts supplemented with 50nM Hi1a trended towards increased LDH release compared to hearts supplemented with 10nM Hi1a or unsupplemented cardioplegia, however this difference was no longer present following 30 minutes reperfusion (Figure 2).
Conclusions: Supplementation of Celsior with Hi1a showed improved cardiac function after 6 hours cold ischaemic storage in a dose-dependent manner, showing benefit as a preconditioning agent. Increased LDH release with increasing Hi1a dose may indicate possible adverse effects with high-dose Hi1a despite functional improvement. Further work is needed to examine reasons for differing efficacy in different cardioplegia solutions and possible mechanisms of myocardial necrosis. ASIC1a inhibitors may improve acceptable ischaemic times for organ transplantation however compatibility with various cardioplegia solutions should be considered.
Sanjay Dutta is supported by an Australian National Health and Medical Research Council (NHMRC) Postgraduate Scholarship (2030847).
[1] Donor organ preservation
[2] Heart
[3] Organ perfusion and preservation
