Post-transplant diarrhea: Is there a need for center specific protocol
Arpita Chaudhury(Lahiri)1, Taniya Bhuinya1, Koushik Bhattacharya 1, Atanu Pal1, Sanjay dasgupta 1, Arunangshu Banerjee1.
1Nephrology , NBMCH and IPGMER, Kolkata , India , Kolkata , India
Introduction: Post transplant diarrhea is a common but often neglected complication affecting the quality of life and graft outcome adversely. We report here a study from Eastern India showing the etiopathogenic spectrum of posttransplant population with diarrhea and short-term patient and graft outcome.
Methods: The study is a hospital based single center prospective study with 1 year ( 2021 October to September 2022)inclusion period and minimum 6 month follow up. On top of routine investigation and stool R/E, stool multiplex PCR, colonoscopy with biopsy and CMV DNA PCR were done as per clinical indication. Acute, acute persistent and chronic diarrhea ware defined as per WHO criteria. Renal biopsy was done during follow up as per standard indication.
Results: Among 103 post -transplant follow up patients, 52 patients had 68 episodes of diarrhea and 26 patients required hospital admission. Pain abdomen, fever, bloody diarrhea, watery diarrhea with stool frequency > 10/day, hypovolemic shock with or without AKI at presentation were more associated with infectious diarrhea. Chronic diarrhea, vomiting with anorexia, weight loss were more common in noninfectious diarrhea. Positive yield from stool r/e was only 23%, a stool multiplex PCR yielded positive result in 93% (with 60% revealing multiple organisms). 96% were on standard triple immunosuppression. Any age group, gender, water source, induction therapy did not come out as significant risk factors for infectious diarrhea. While 62% had proven infection, 15% was drug associated and 23% had both issues. 54% had acute diarrhea,23% persistent and 23 % chronic diarrhea. 38 % presented with diarrhea within 6 months. Early presenters had longer hospital stay, more episodes of UTI, and received more targeted therapy for infectious diarrhea with CNI dose modification. Most commonly found organisms were EPEC(17%), Clostridium difficile (14%), Cryptosporidium( 14%),Giardia (14%), Norovirus (6%) and CMV in 2 patients. 54% of hospitalized patients had AKI, but no mortality. Risk of AKI was significantly higher in patients with prior history of rejection in preceding 6 months. (Figure 1)
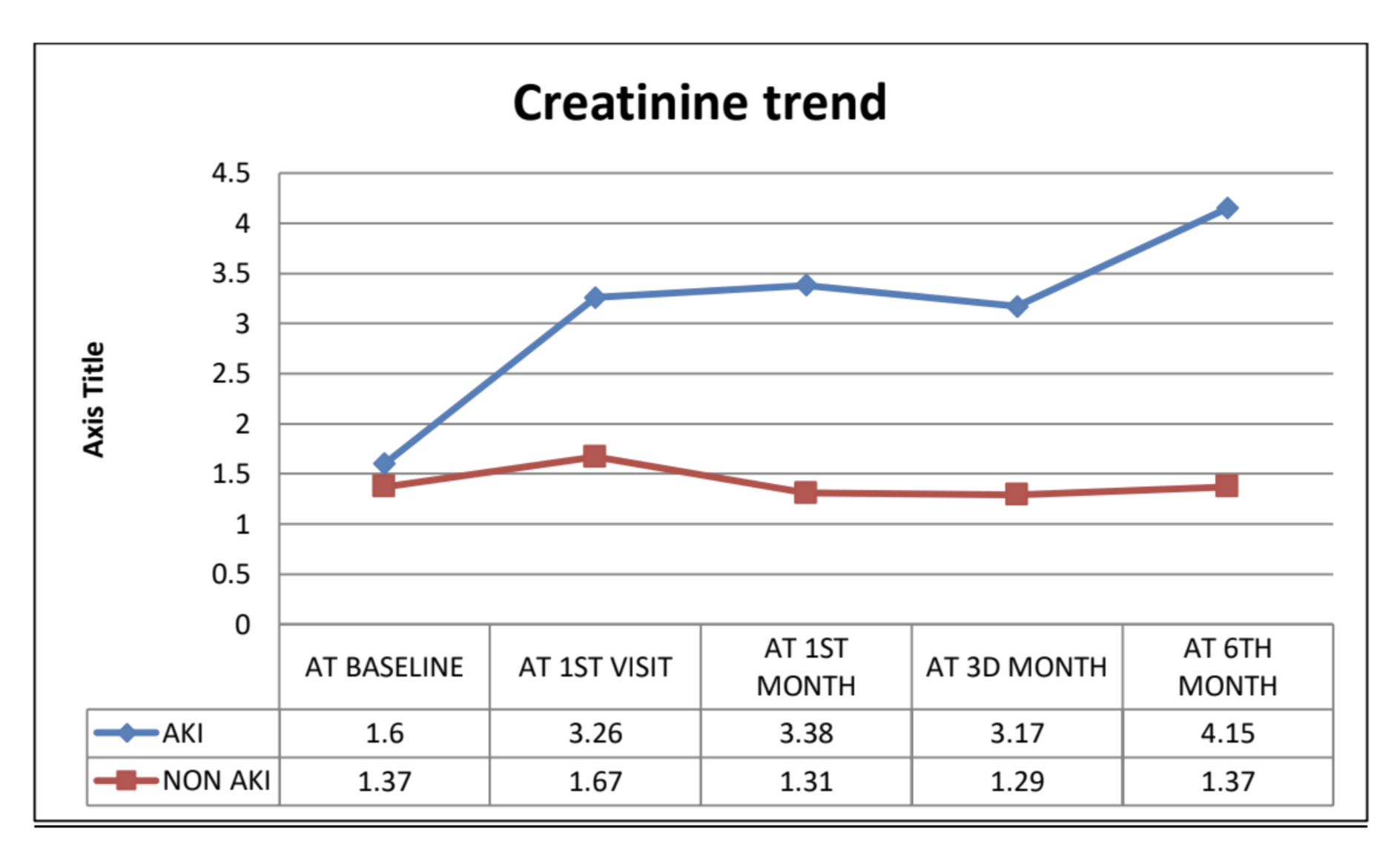
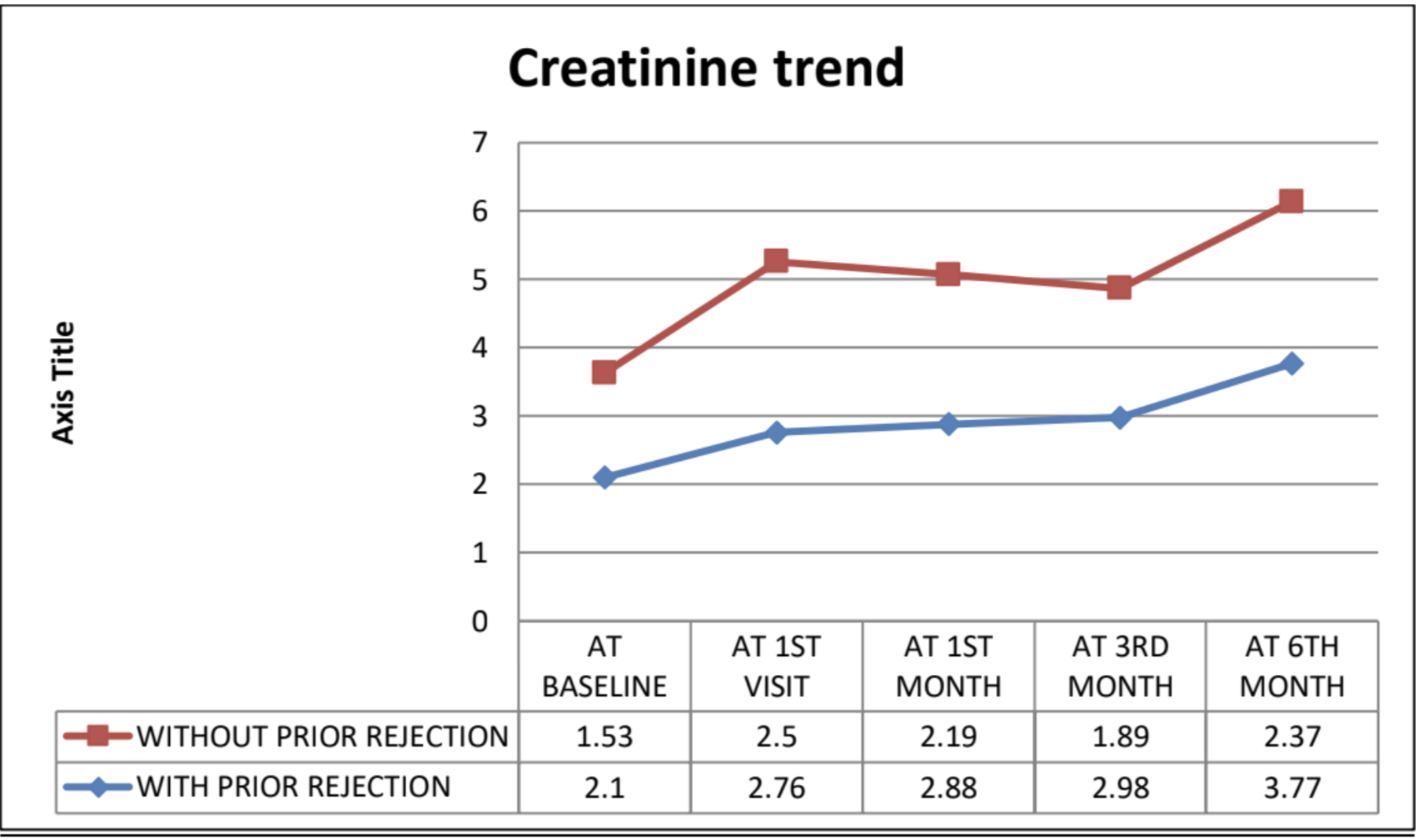
44% of post diarrheal AKI needed dialysis. Among HD requiring patients persistent graft dysfunction was seen in 50% of patients at 6 th month with biopsy confirmed chronic allograft injury. (Figure 2)
Conclusion: The reported multifactorial chronic graft dysfunction in patients following diarrhea with AKI, with a non-identical aetio-pathogenic spectrum when compared to reports from other centers of India, underscores the need for more regional reports and framing of center specific diagnostic algorithm for post-transplant diarrhea.
