Hikaru Aoki, Japan has been granted the TTS-JST Basic and Translational Mentee-Mentor Award
Adverse effects of graft congestion and ameliorative effects of hepatocyte growth factor after liver transplantation in rats
Hikaru Aoki1, Takashi Ito1, Masaaki Hirata1, Shinya Okumura1, Yuki Masano1, Eri Ogawa1, Hironori Haga2, Etsuro Hatano1.
1Department of Surgery, Kyoto University, Kyoto, Japan; 2Department of Diagnostic Pathology, Kyoto University, Kyoto, Japan
Introduction: Living-donor liver transplantation and deceased-donor split-liver transplantation often result in congested areas in liver grafts. The regeneration and function of congested areas, especially in liver grafts, remain unclear. Therefore, we aimed to investigate the regeneration and function of congested areas after liver resection and liver transplantation and explore a new approach to improve the effects of graft congestion.
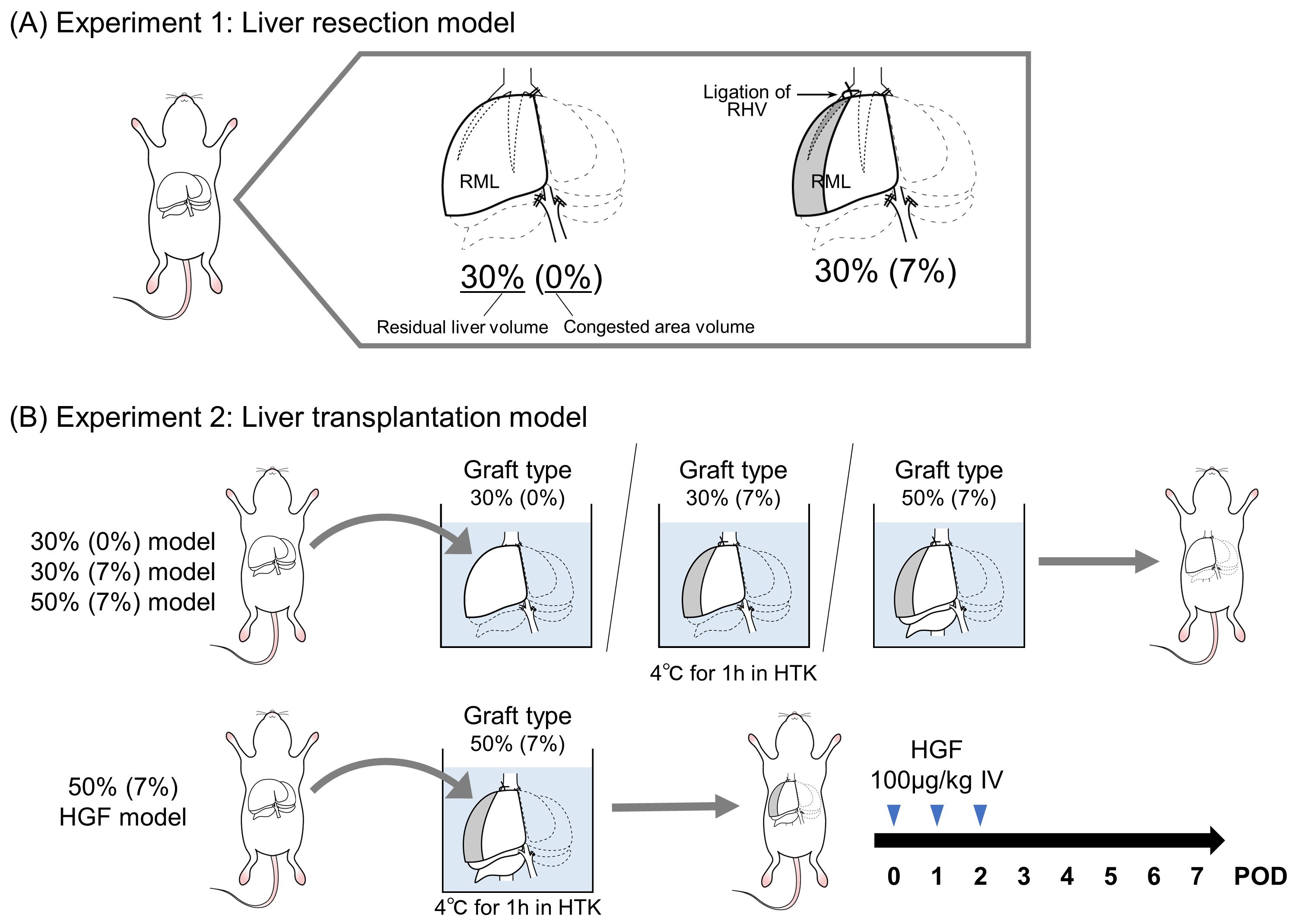
Method: We created new rat models with congested areas in the partial livers by liver resection and ligation of the right hepatic vein (RHV). We orthotopically transplanted those livers into syngeneic rats. Ligation of RHV resulted in congested area in approximately 7% of the whole liver.
Experiment 1: Liver resection model (Figure 1A).
The 30% residual liver (the right median lobe [RML]) model with ligation of RHV was defined as the 30% (7%) model. The 30% residual liver model without ligation of RHV was defined as the 30% (0%). We compared the postoperative outcomes between the two groups.
Experiment 2: Liver transplantation model (Figure 1B).
In addition to 30% (0%) and 30% (7%) models, the 50% residual liver (RML and the right lobe) model with ligation of RHV (50% [7%] model) was used as a graft. Additionally, some rats in the 50% (7%) model received recombinant human hepatocyte growth factor (HGF) administered at 100 µg/kg immediately after transplantation and on postoperative (POD) 1 and POD2. The 50% (7%) model with HGF administration was defined as the 50% (7%) HGF model.
Results: In the liver resection model, all rats in the 30% (0%) and 30% (7%) models survived until POD7. In 30% (7%) model, the microscopic findings showed hepatocyte loss in the congested area on POD1; however, the congested area recovered to completely normal on POD7 (Figure 2A). In the transplantation model, while the survival rate of the 30% (0%) model was 100%, no rats in the 30% (7%) model could survive until POD3 (Figure 2B). The 50% (7%) model also exhibited a significantly worse survival rate than the 30% (0%) model (p=0.039), even though the 50% (7%) model had a larger normal (non-congested) volume than the 30% (0%) model. Some congested areas in the 50% (7%) model exhibited necrosis and abscesses on POD7 (Figure 2C, yellow triangles). The survival rate of the 50% (7%) HGF model was 100% and significantly better than that of the 50% (7%) model (p=0.039) (Figure 2B). The 50% (7%) HGF model exhibited significantly fewer necrotic areas in the congested area than the 50% (7%) model on POD7 (p<0.05) (Figure 2C).
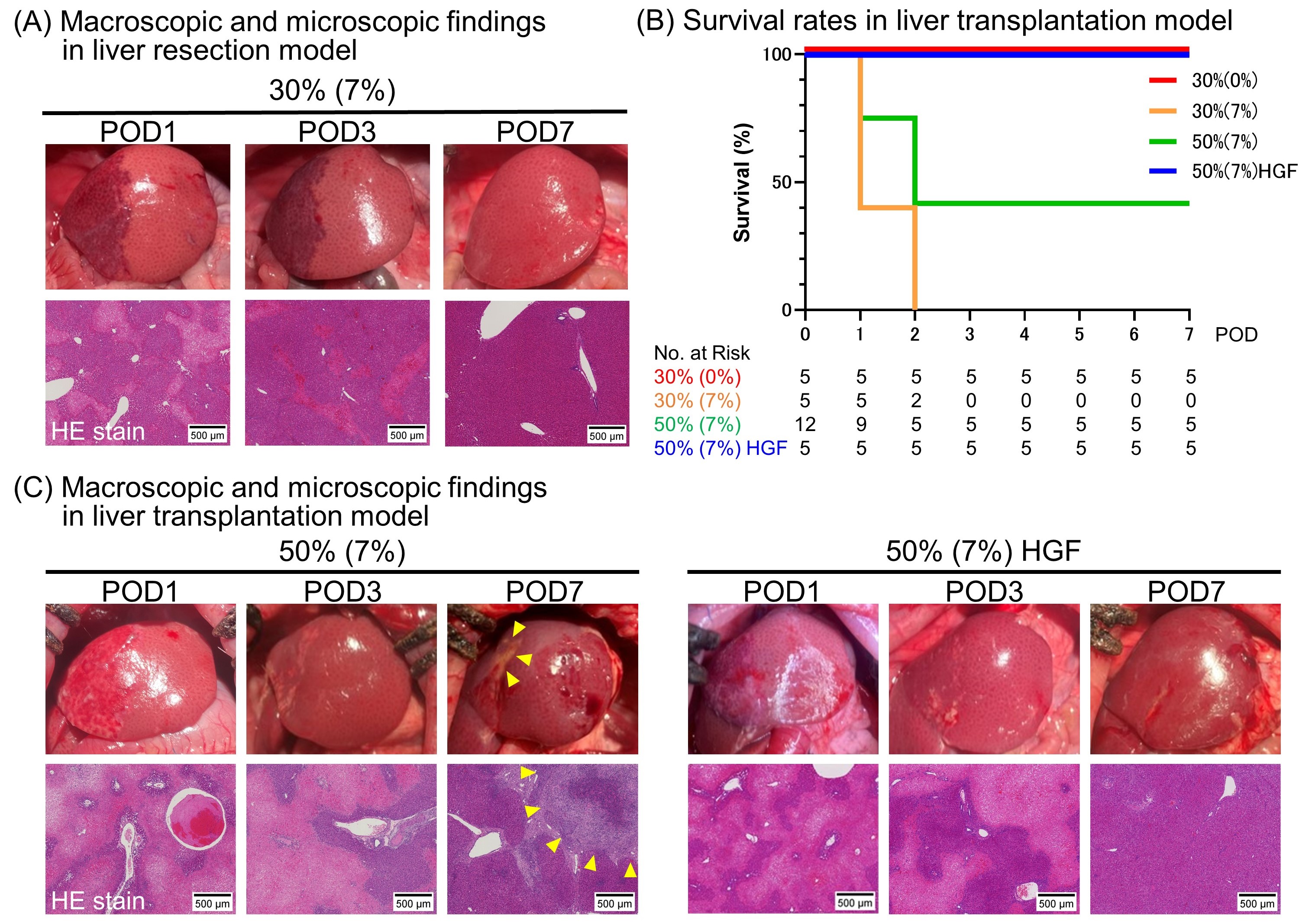
Conclusion: Although congested areas after liver resection regenerated normally in rats, congested areas of liver grafts caused necrosis. Adding congested areas to liver grafts may have a negative impact on recipients. Short-term administration of HGF can ameliorate the function and regeneration of congested areas of liver grafts and improve postoperative outcomes.
[1] Graft Congestion
[2] Liver Transplantation
[3] Liver Regeneration
[4] Hepatocyte Growth Factor
[5] Rat
