
Phenotype of interstitial inflammation and tubulitis in mixed rejection compared to T cell mediated rejection: A study using CODEX multiplex imaging and machine learning
Angelica Perez-Gutierrez1, Madeleine S Durkee2,3, Junting Ai3, Gabriel Casella2,3, Thao Cao4, Anthony Chang5, Michael S Andrade1, Beatriz Concepcion3, Dustin Shaw6, John J Fung1, Rolf N Barth1, Maryellen L Ginger2, Marcus R Clark3, Anita Chong1.
1Surgery, University of Chicago , Chicago, IL, IL, United States; 2Radiology, University of Chicago , Chicago, IL, IL, United States; 3Medicine, University of Chicago , Chicago, IL, IL, United States; 4Pathology, University of Chicago , Chicago, IL, IL, United States; 5Pritzker School of Molecular Engineering, University of Chicago , Chicago, IL, IL, United States; 6Pritzker School of Medicine, University of Chicago , Chicago, IL, IL, United States
Introduction: Kidney transplantation is considered the optimal treatment for kidney failure, yet graft survival is often compromised by rejection. Rejection can manifest as T-cell mediated rejection (TCMR) or antibody-mediated rejection (ABMR). When biopsy results reveal characteristics of both types, the condition is referred to as mixed rejection (MR). It remains unclear whether mixed rejection represents a combination of TCMR and ABMR or if it constitutes a separate pathological entity. Notably, mixed rejection is associated with poorer outcomes compared to either ABMR or TCMR alone. In this study, we aimed to compare the interstitial inflammation and tubulitis observed in mixed rejection compared to TCMR alone.
Methods: We conducted co-detection by indexing (CODEX) multiplex imaging on nine graft biopsies from cases of TCMR (Banff 1A) and 12 from cases of MR). We used a panel of 44 markers that defined renal cells and CD45+ immune infiltrate.
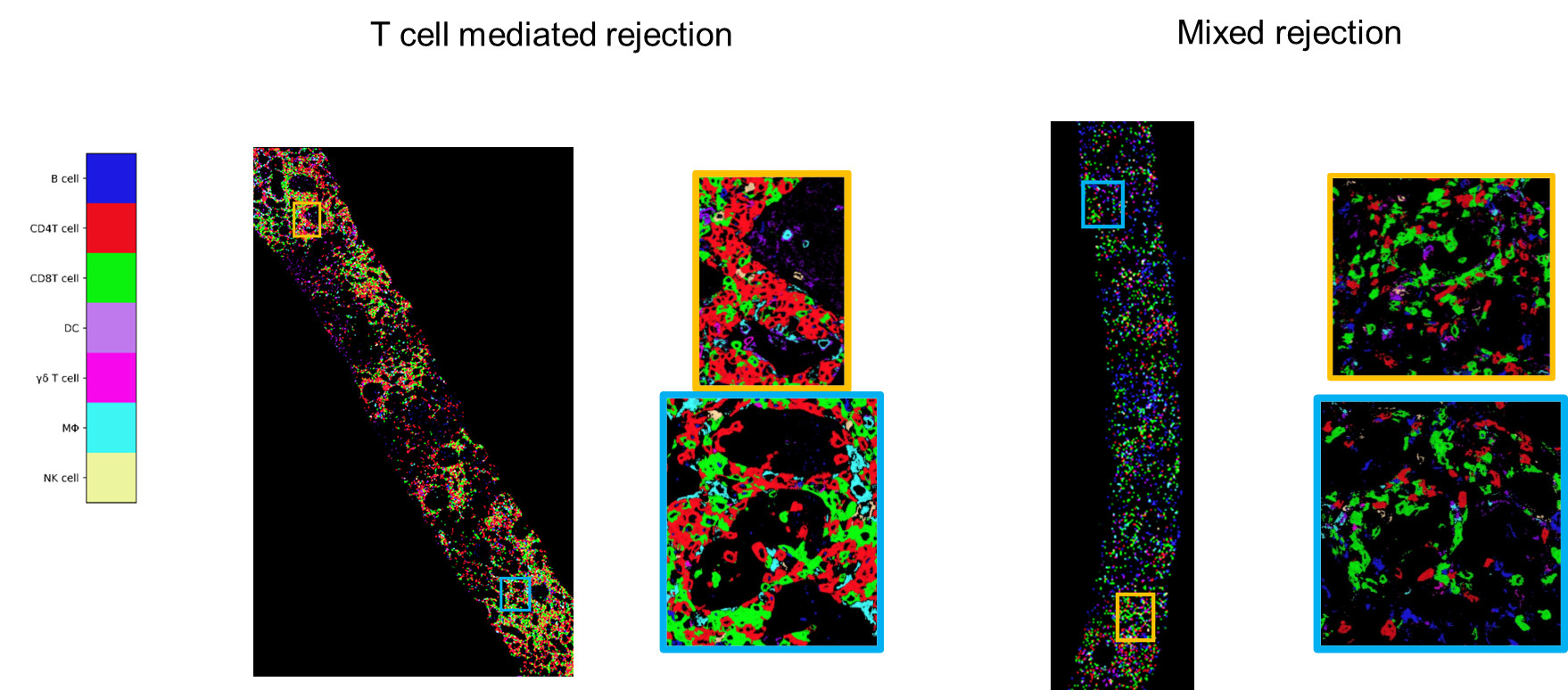
We classified CD4+ T cells, CD8+ T cells, gamma delta (γδ) T cells, B cells, macrophages, natural killer (NK) cells, and dendritic cells (DC); all renal cells and remaining immune cells were labeled as ‘unclassified’. Tubules were segmented using a custom Omnipose model. Our analysis focused on defining these specific immune cells in two anatomical compartments: interstitium and tubules.
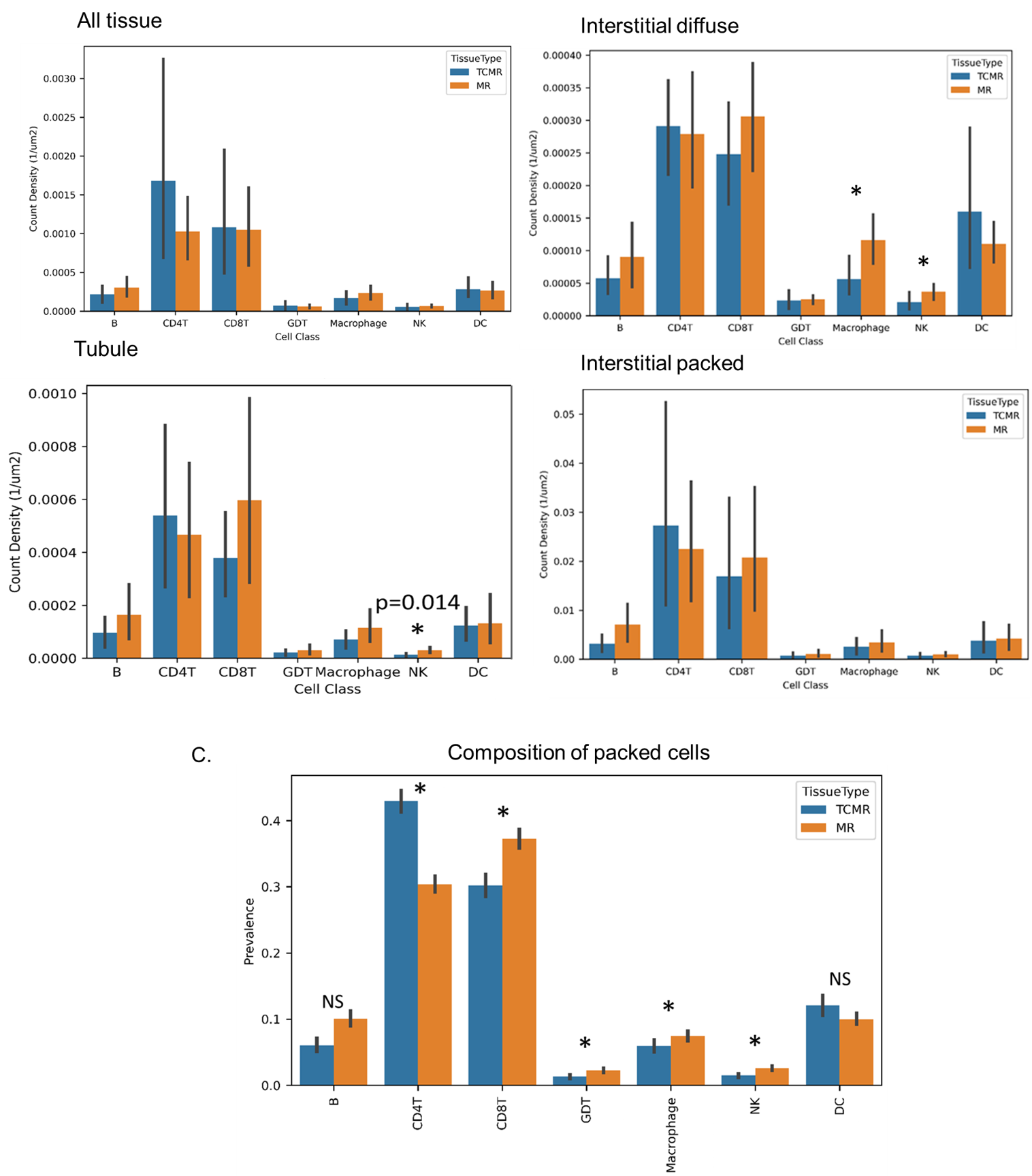
Results: There were no significant differences in the immune cell composition between TCMR and MR biopsies overall. However, within the tubules, NK cells displayed a significantly higher count density in MR compared to TCMR, even though overall counts were low. Similarly, no significant differences were observed in the cell density of the overall interstitial infiltrate between the two conditions.
Analysis of the composition of densely packed cells in the interstitium revealed that TCMR biopsies contained significantly higher proportions of CD4+ T cells than those in MR biopsies (p<0.001). Conversely, packed cells in MR demonstrated significantly higher proportions of CD8+ T cells (p<0.001), γδ T cells (p=0.01), macrophages (p=0.002), and NK cells (p=0.001), and a trend towards higher proportions of B cells, compared to those in TCMR compared to those in TCMR.
HLA II expression was significantly higher in macrophages and DC's in MR than in TCMR, and conversely, significantly higher in B cells in TCMR compared to MR.
Conclusions: Comparison of the cellular infiltrate in TCMR and MR showed broad similarities but some significant differences, including the preponderance of CD4+ T cells in TCMR and CD8+ T cells in MR. Ongoing studies are testing whether cognate interactions of CD4+ or CD8+ T cells with HLAII+ B cells, DCs and macrophages differ between MR and TCMR. These studies will lead to understanding the interactions driving MR vs TCMR, and point to new approaches for treatment. Future directions will compare the phenotype of the interstitial infiltrate with antibody-mediated rejection.
[1] CODEX
[2] Mixed rejection
[3] T-cell mediated rejection
[4] Immune phenotype
