
Effect of donor-recipient height and gender disparity on kidney transplant outcome: Analysis of the Thai transplant registry
Chumpol Santisiripat1, Korntip Phonphok 1.
1Division of Nephrology, Department of Internal Medicine, Rajavithi Hospital, Bangkok, Thailand
Introduction: Transplantation of a relatively smaller kidney donor to recipient size, combined with an additive effect of gender mismatching, may result in glomerular hyperfiltration injury due to nephron underdosing. This could potentially lead to suboptimal graft outcomes. Given the strong correlation between height and gender with kidney morphology, we hypothesized that kidneys of donor (D)-recipient (R) height and gender disparity would have inferior short- and long-term graft and patient outcomes.
Method: We conducted a retrospective cohort study using data from the Thai Transplant Registry. Adult patients ≥18 years underwent living and deceased donor kidney transplantation (LDKT and DDKT) between 1987 and 2021, with available R and D height data, were included. We categorized D-R height pairings into 3 groups based on a 10-centimeter (cm) height difference (recipient ≥10cm taller than donor [R>D], recipient within 10cm shorter or taller than donor [R=D] and recipient ≥10cm shorter than donor [R<D]), and gender pairings into gender identical and gender disparity. The primary outcome was 1-year, 5-year, and 10-year death-censored graft survival (DCGS). Secondary outcome was overall patient survival following KT. Demographic data were analyzed using Chi-squared test, Fischer's exact test, and analysis of variance (ANOVA). Outcome measures were investigated using Kaplan–Meier survival analysis and the Cox proportional hazard model. Firth penalized Cox regression was also implemented. This study was approved by Rajavithi Hospital ethics committee.
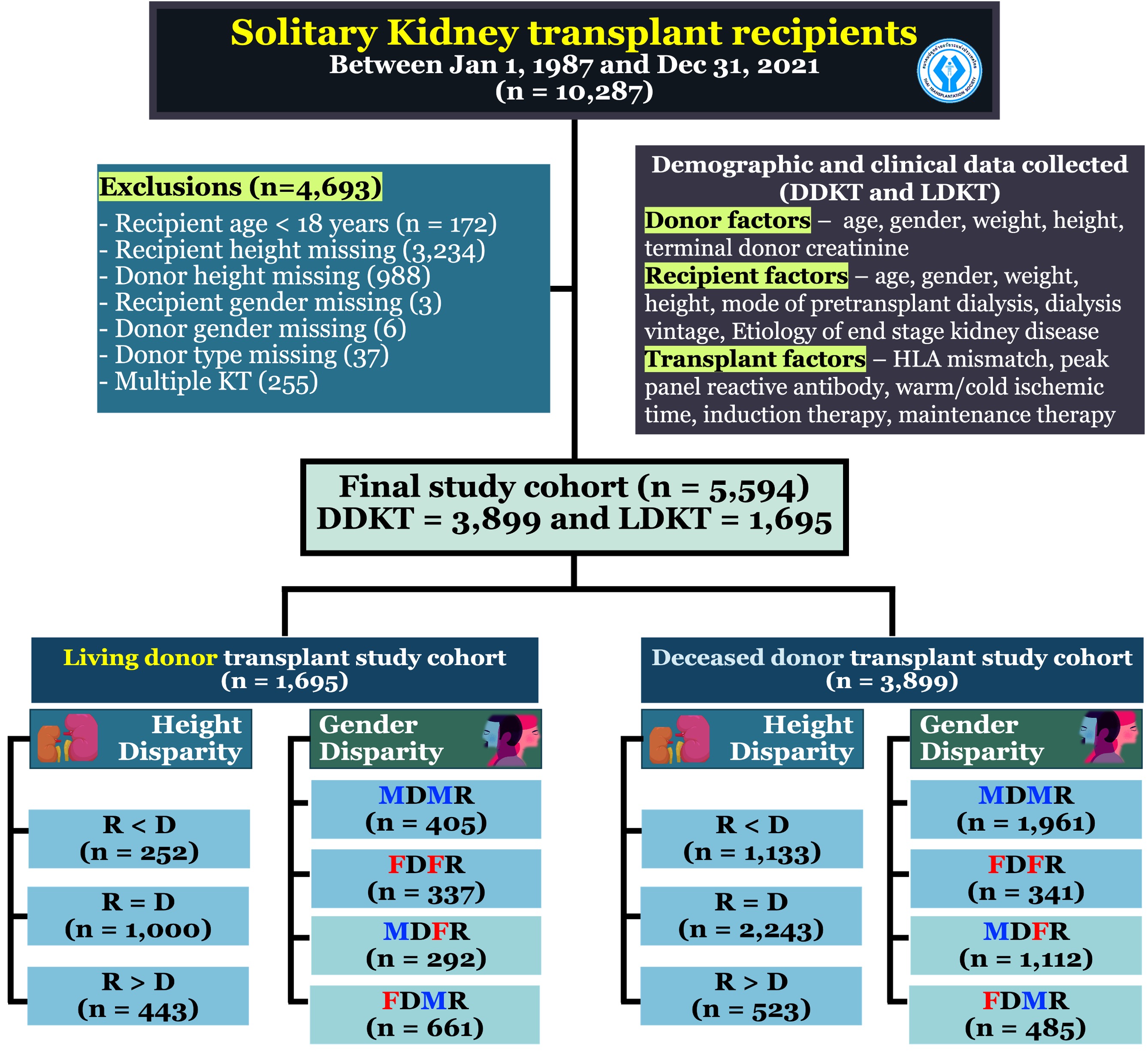
Results: The data revealed a total of 5,594 transplants, with 1,695 being LDKT and 3,899 being DDKT. Of these, the R<D group exhibited the highest 10-year DCGS following LDKT (R<D: 93.87%, R=D: 83.13% and R>D: 76.75%; p=0.01) and DDKT (R<D: 77.18%, R=D: 75.58% and R>D: 67.67%; p=0.04). We also found superior 5-year patient survival among gender disparity group following DDKT (92.79% vs 90.47%; p=0.04). However, after adjusting for covariates, multivariate Cox regression analyses revealed no significant association.
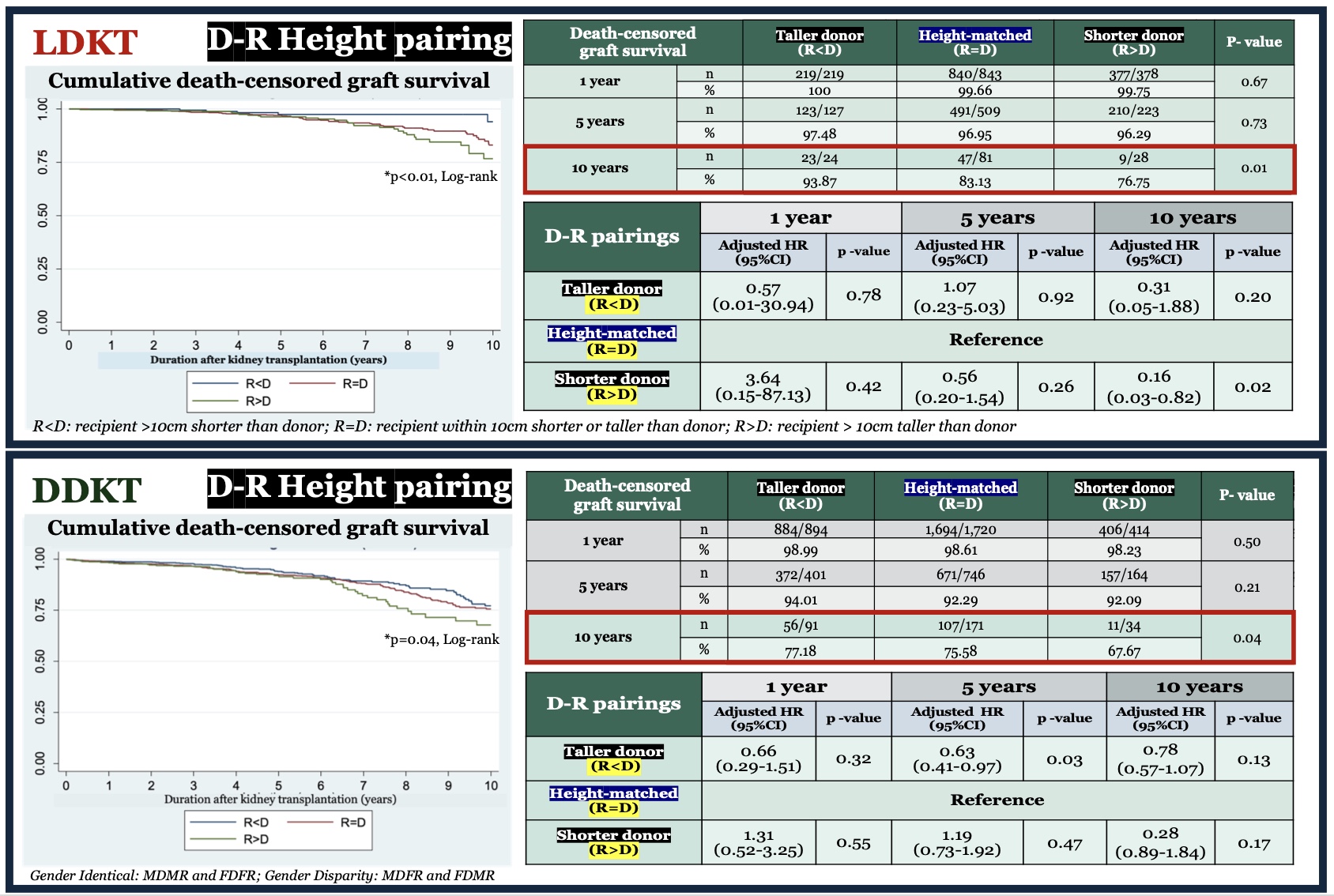
Conclusion: D-R height and gender disparity were not associated with DCGS and overall patient survival among Thai living- and deceased-donor KT population. In determining the long-term outcome following KT, donor kidneys should not be rejected based on the height or gender difference, particularly in DDKT.
All kidney transplant centers in Thailand for data contribution to the Thai Transplant Registry. The ethics committee, Rajavithi Hospital for research funding.
[1] Height Disparity
[2] Gender Disparity
[3] Kidney Transplant Outcome
[4] Death-Censored Graft Survival
[5] Patient Survival
