Surgical modifications to the conventional kidney transplant technique - The Miami transplant institute approach
Gaetano Ciancio1,2,3, Marina Tabbara1,2, Javier Gonzalez4, Angel Alvarez1,2, Mahmoud Morsi 1,2, Jeffrey Gaynor1,2.
1Miami Transplant Institute, Jackson Memorial Hospital, University of Miami Miller School of Medicine, Miami, FL, United States; 2DeWitt Daughtry Family Department of Surgery, University of Miami Miller School of Medicine, Jackson Memorial Hospital , Miami, FL, United States; 3Department of Urology, University of Miami Miller School of Medicine, Jackson Memorial Hospital, Miami, FL, United States; 4Department of Urology, Hospital General Universitario Gregorio Marañón, Madrid, Spain
Background: Limited improvements/refinements of the conventional surgical technique in kidney transplantation have been reported over the years. Thus, surgical complications may still occur post-transplant and are associated with unfavorable outcomes, including recurring morbidity, repeat hospitalizations, and potentially even graft failure or death. Over the past 20 years at our center, surgical modifications to the conventional kidney transplant technique were developed with two goals in mind: to minimize the risk of developing post-transplant urologic/vascular/other surgical complications, and to simultaneously eliminate the need for initial ureteral stent placement and surgical drainage.
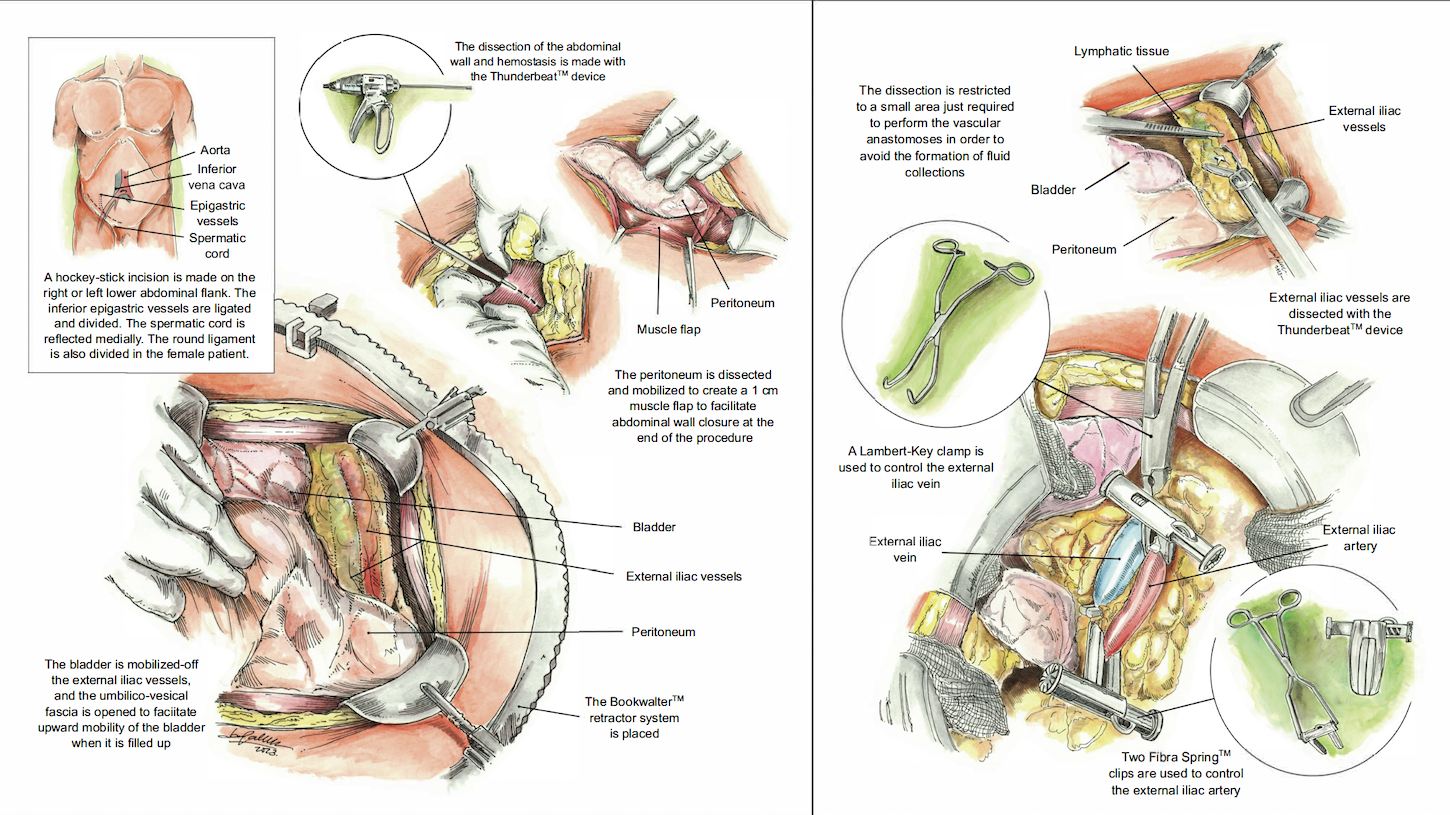
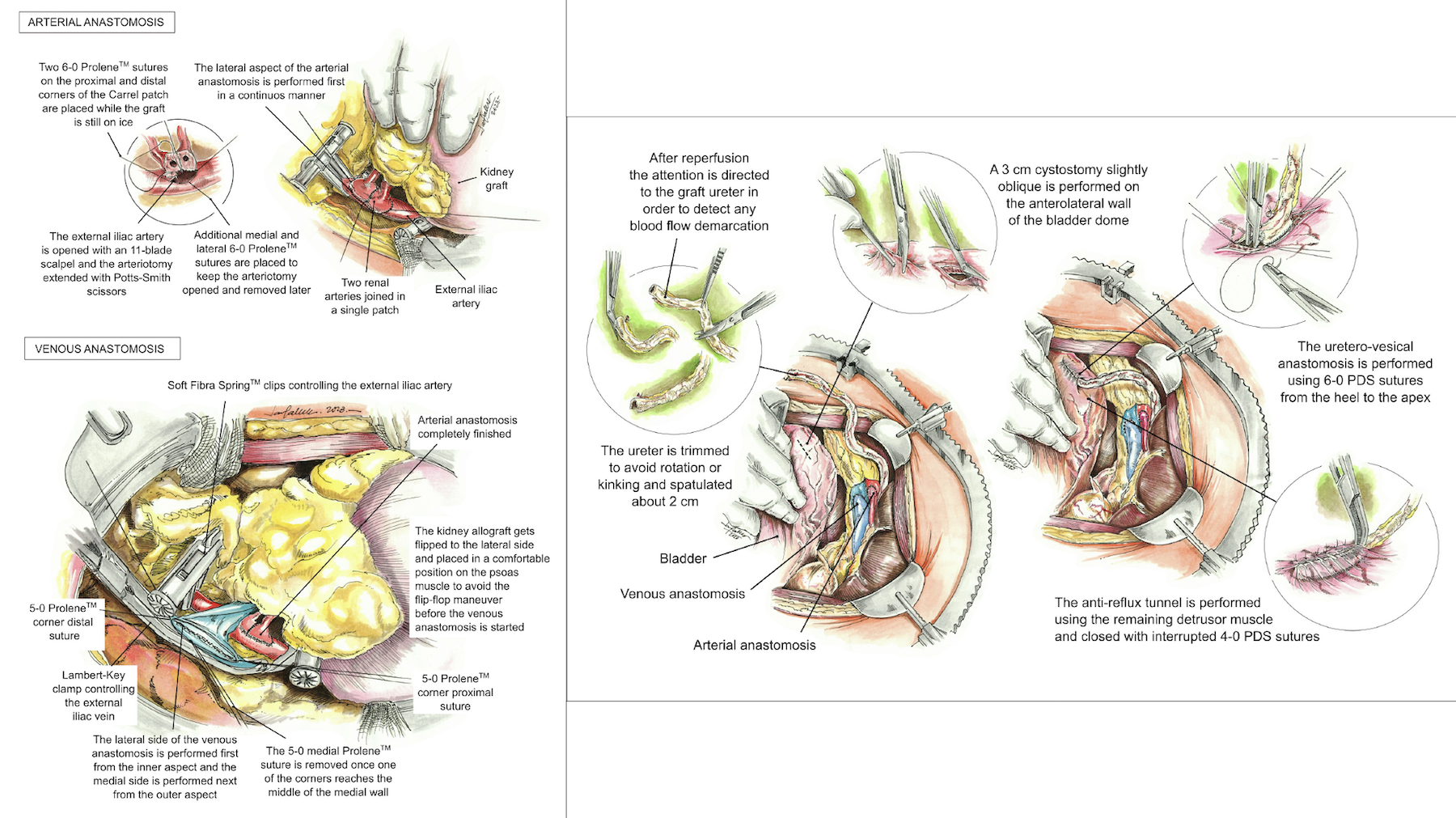
Methods: Here, we describe these modifications along with(what we believe are) their advantages over the conventional technique: creating an abdominal flap for easier abdominal closure(reflecting the parietal peritoneum from the abdominal wall), mobilizing the bladder before transplant(creating more space for bladder dissection, allowing it to move upward during abdominal wall closure), minimizing the dissection of iliac vessels to only anterior lymphatic tissue(attempting to minimize the incidence of fluid collections), using plastic arterial vascular bulldog clamps(causing less trauma to the iliac artery), performing vascular anastomosis of the renal artery first(making it easier for the surgeon to perform this anastomoses), creating longer ureteral spatulation, and inclusion of bladder mucosa along with some detrusor muscle layer in performing the ureteral anastomosis(attempting to minimize the incidence of urologic complications), and no initial use of ureteral stent placement or surgical drainage. We report our experience during the first 12mo post-transplant of a single transplant surgeon(G.C.) who used each of these modifications among 707 consecutive recipients of kidney-alone transplants at our center since 2014. All patients were followed for a minimum of 12mo post-transplant.
Results: During the first 12mo post-transplant, 2.3%(16/707) of patients developed a urologic complication; only 1.0%(7/707) required surgical repair of their original ureteroneocystostomy. Additionally, 2.7%(19/707) developed a vascular complication; 8.8%(62/707) developed some other type of surgical complication(wound complication, lymphocele development, or development of a peri-renal hematoma or peri-renal collection). These overall results were clearly advantageous when compared with other studies.
Conclusion: We believe that this modified kidney transplant technique clearly helped in reducing post-transplant risks of developing urologic/vascular/other surgical complications. Importantly, these results were achieved without initial ureteral stent placement or surgical drainage.