Perfusion techniques and long-term outcomes in kidney transplantation: A systematic review and meta-analysis
Bima Hasjim1, Jes M Sanders2, Michael Alexander1, Robert R Redfield III1, Hirohito Ichii1.
1Surgery, UC Irvine, Orange, CA, United States; 2Surgery, Northwestern University, Chicago, IL, United States
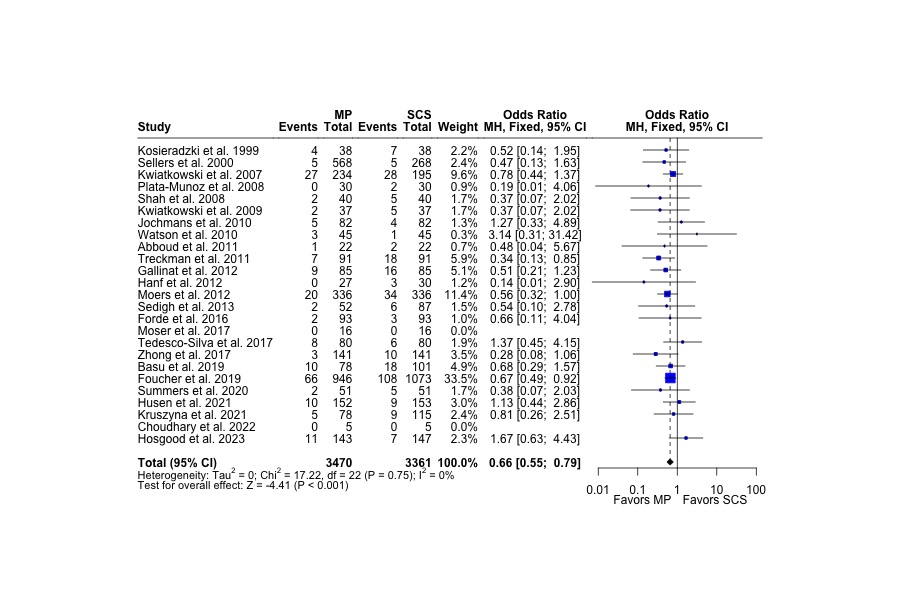
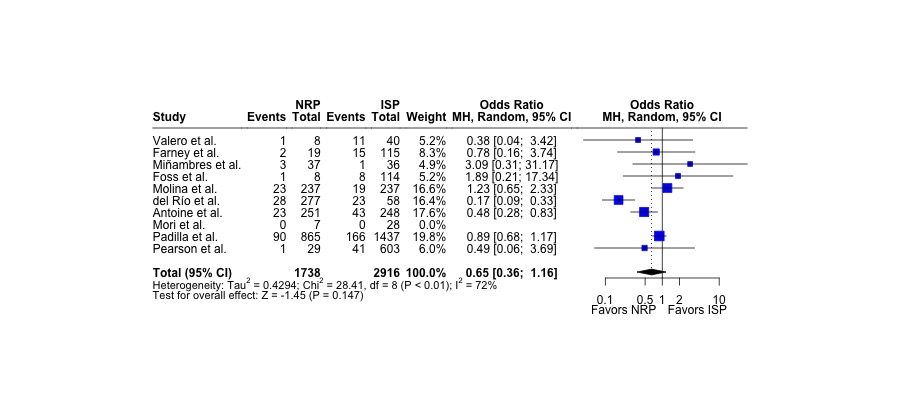
Kidney transplantation is the only definitive treatment for chronic kidney disease and high risk allografts are increasingly used to expand the donor pool. Machine perfusion (MP) and normothermic regional perfusion (NRP) techniques for organ preservation have been developed to mitigate ischemic reperfusion injury (IRI) in allografts. While the benefits in short-term graft function have been documented, long-term outcomes have been more challenging to investigate. We performed a systematic review and meta-analysis to examine the benefits of MP and NRP compared to traditional organ preservation techniques in kidney transplantation. PubMed (MEDLINE), Embase, Cochrane, and Scopus databases were queried and, of 13,794 articles identified, 54 manuscripts were included (N=41 MP articles; N=13 NRP articles). Among MP studies, 10 (24.4%) were retrospective studies, 17 (41.5%) were prospective studies, and 14 (34.2%) were randomized control trials. The NRP literature were made up of 6 (46.2%) retrospective studies and 7 (53.8%) prospective studies, but no (0%) randomized control trials. MP grafts had longer CIT (15.2 hours vs. 13.3 hours, P=0.011), WIT (33.9 minutes vs. 30.8 minutes, P=0.016), and higher terminal donor serum creatinine (1.16 mg/dL vs. 1.09 mg/dL, P=0.030) compared to static cold storage. MP decreased the rates of 12-months graft failure (OR 0.67; 95%CI 0.55, 0.80; P<0.001) as well as other perioperative outcomes such as delayed graft function (OR 0.65; 95%CI 0.54, 0.79; P<0.001), primary nonfunction (OR 0.63; 95%CI 0.44, 0.90; P=0.011), and hospital length of stay (15.5 days vs. 18.4 days; P=0.009). In contrast, NRP had similar rates of 12-months graft failure (OR 0.65; 95%CI 0.36, 1.16; P=0.147), delayed graft function (OR 0.80; 95%CI 0.42, 1.54; P=0.507), and primary nonfunction (OR 0.74; 95%CI 0.40, 1.39; P=0.355) compared to in situ cold preservation. However, NRP had reduced the rates of acute rejection (OR 0.48; 95%CI 0.35, 0.67; P<0.001). Overall, dynamic preservation techniques can overcome the risks of lower quality allografts and improve short- and long-term function compared to traditional storage practices. MP and NRP can play an important role in safely expanding the donor pool to satisfy the increasing demands of kidney transplantation.
[1] Machine perfusion
[2] Normothermic regional perfusion
[3] Ischemic reperfusion injury
[4] Organ preservation
[5] in situ cold preservation
[6] static cold storage
[7] kidney transplant
