En bloc kidney transplant to pediatric recipient: Experience of a tertiary care hospital
Eduardo Angulo1, Brenda G Becerra1, JImena D Del Villar1, Yuridia L Plascencia1, Soledad Zarate1, Gabriela Hermosillo1, Alfonso Navarro1, Jose M Zertuche1, Nidia M Arreola1, Bettina Torres1, Jose E Ortiz1, Daysi C Gónzalez 1.
1Servicio de Trasplante Renal Pediátrico, Instituto Mexicano del Seguro Social , Guadalajara, , Mexico
Trasplante Pediátrico de Occidente.
Introduction: Kidney transplant is the best therapeutic option for children with end-stage chronic kidney disease (CKD). In Mexico, there is a great demand for organs for transplant, with organs from deceased donors under 5 being considered. years for pediatric recipients, without being accepted in adults for small renal masses. En bloc transplantation presents a higher risk of complications; in recent decades, due to improvements in surgical techniques and immunosuppressive therapy, its incidence has decreased in transplant patients, leading to better long-term survival and quality of life.
Objective: Report the Survival of patients with en bloc kidney transplants, 18 years of experience in a pediatric hospital in Western Mexico.
Material and methods: 21 en bloc transplants performed from 2006 to 2023 were included. It is a longitudinal, analytical, retrospective study. The variables studied were: demographic characteristics of the donor and recipient, surgical event and technique, clinical evolution of the recipient at 1 and 5 years post-transplant; with follow-up to date to determine patient and graft survival. The statistical analysis was: frequencies, percentages, Xi2 and Kaplan Meier.
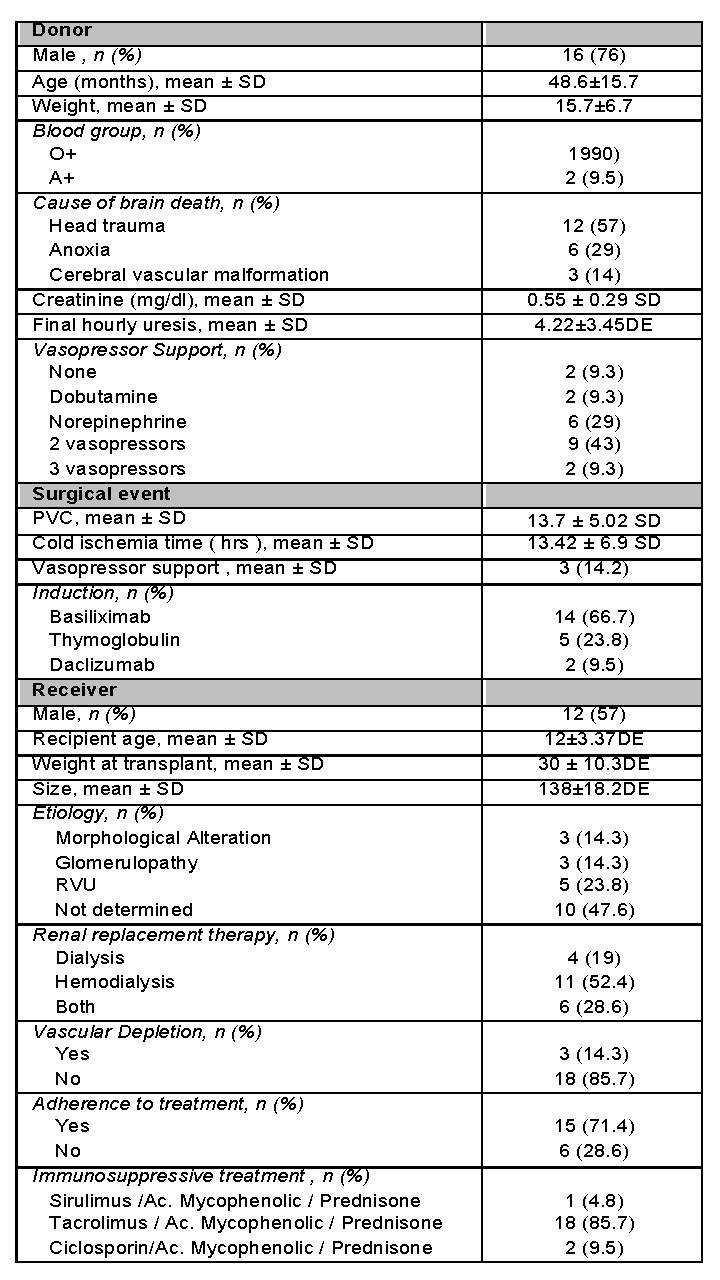
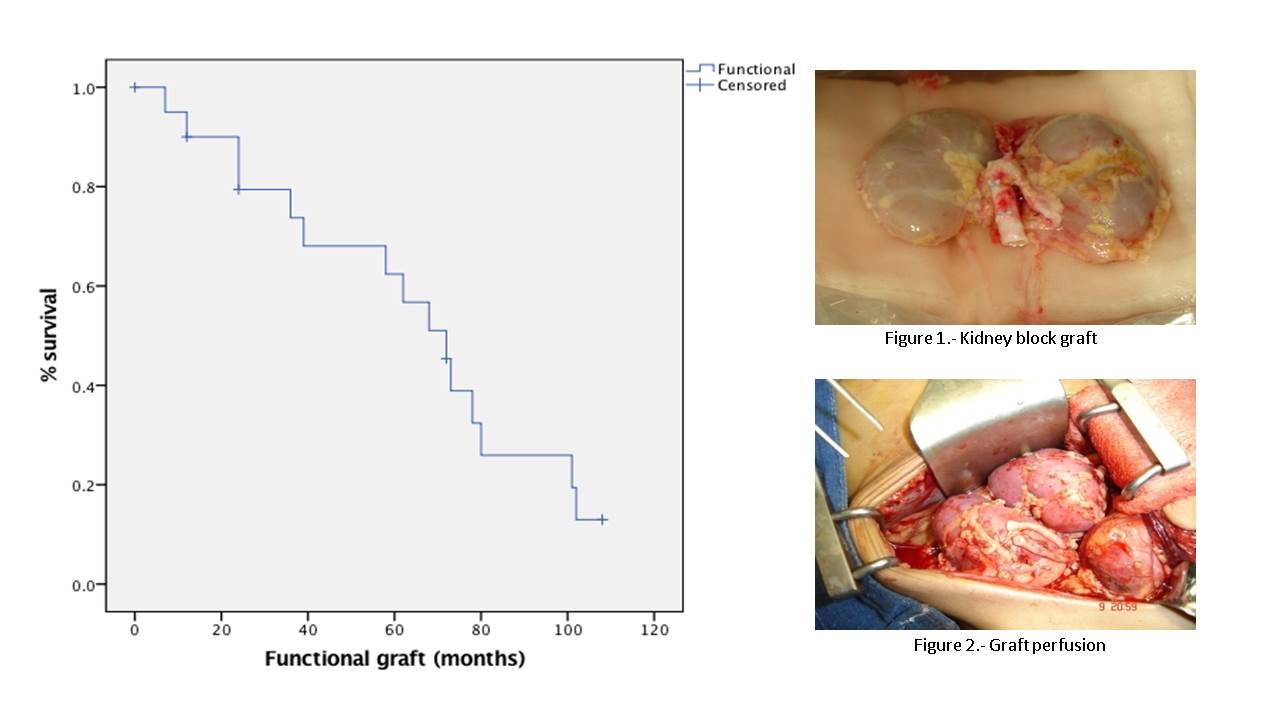
Results: The mean age of the donor was 48 months ( ± 33.7 SD ), the main cause of brain death was head trauma, confirmed by Angiotomography in 67%. The mean age of the recipient was 12 years ( ± 3.3 SD), with unknown etiology of kidney disease (48%); The average length of stay in substitution therapy was 2.9 years. Induction therapy was basiliximab/methylprednisolone (67%). The surgical placement technique was extrabdominal Gibson type with shotgun urethral reimplantation; The cold ischemia time was 13.42 hours ( ± 6.9 SD). Early complications were delayed graft function (33%) and renal thrombosis (9.5%). The late ones were humoral rejection (33%) and infectious complications (38%). The 1st year mortality was 4.6% and the graft survival at one year was 95.3%. Overall graft survival is 63 months (min 12, max 204), with mean creatinine of 0.77mg/dl. The factor associated with graft loss is poor adherence to immunosuppressive treatment (p<0.0001). The 5-year graft survival was 72%.
Conclusions: Pediatric donation of kidneys that are transplanted en bloc are a safe and effective alternative, with excellent short and long-term results, improving the survival and quality of life of children with CKD, candidates for transplant.
