Pediatric liver transplantation in Situs inversus and other vascular abnormalities
Maren Schulze1, Arzu Oeczelik1, Juergen Treckmann1, Simone Kathemann2, Elke Lainka2, Ulf P Neumann1.
1Department of General Visceral and Transplant Surgery, University Hospital Essen, Essen, Germany; 2Dep. of pediatric gastroenerology and hepatology, University Hospital Essen, Essen, Germany
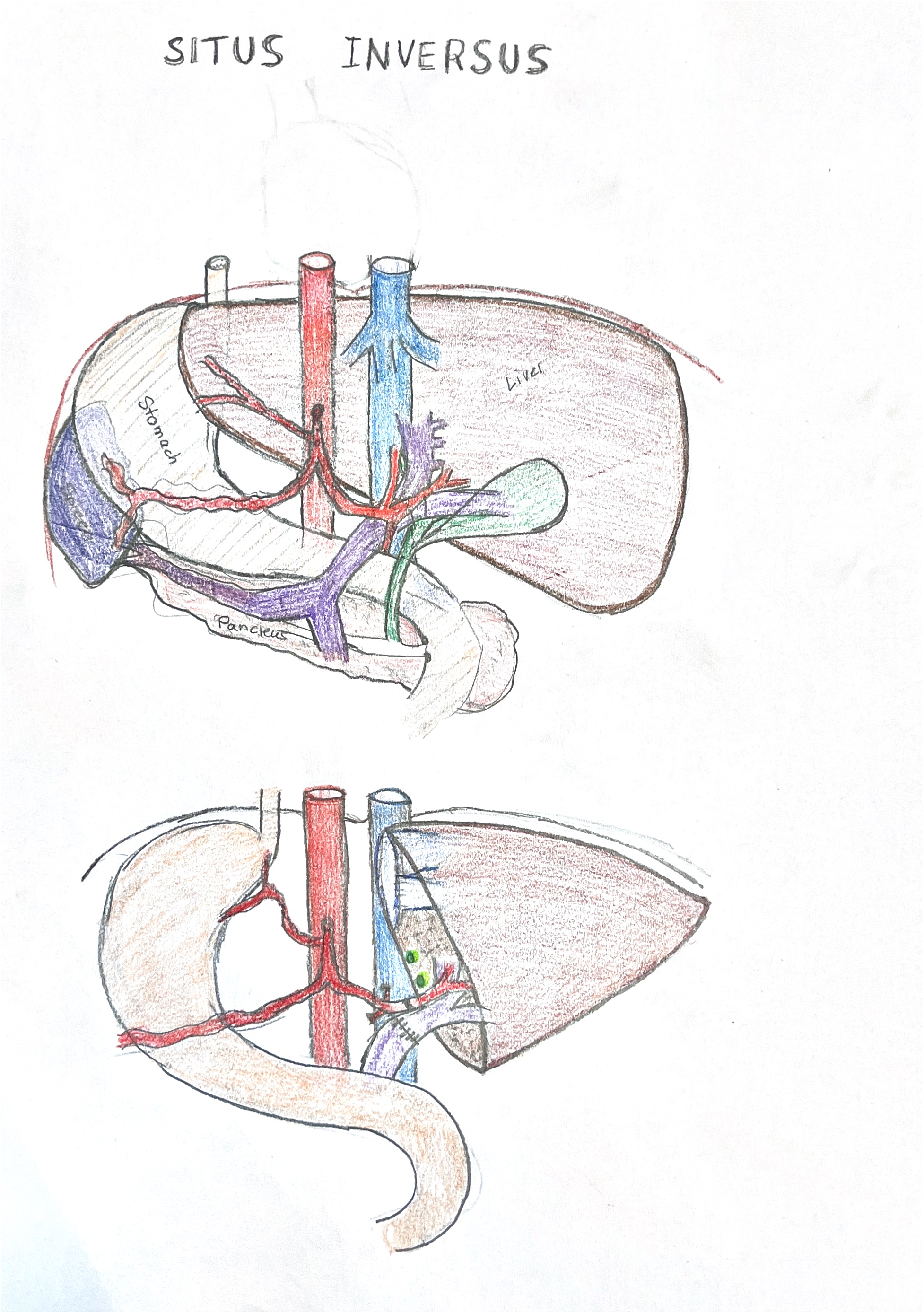
Some cases of biliary atresia can be subcaterozied as syndromatic which means that they coincide with malformations such as situs inversus, isolated dextrocardia and or vena cava aplasia with continuity of vena azgos or hemiazygos.
We here report of two cases with biliary atresia and situs inversus for whom we performed liver transplantation. On our waiting list we have two patients with biliary atresia and vena cava aplasia, one with situs inversus.
The first patient had preious Kasai operation and revision of Kasai operation and was listed with decompensated cirrhosis and acute kidney injury. She also had severe portal vein hypoplasia.
" href="https://app.tts2024.org/papers/body/1574#">
She underwent living related tranplantation from her mother, portal vein anastomosis was done twice for initially insufficient flow and was finally anastomosed to the venous conflues. Arterial reconstruction was difficult, due to the shortness of the artery and had to be placed posterior to the portal vein. On day 12 the patient developed arterial thrombosis and biliary leakage she was re-listed. On day 19 she recieved a split liver transplant reconstructed with an arterial and portal venous jump graft. Abdomen was partially closed at the time of transplant and completely closed after two revisions.
The second patient had previous Kasai operation and was primarily transplanted with a split liver transplant with long vessels, so the arterial recontruction could primarily be positioned anterior to the portal vein.
From previous experiences with vena cava aplasia we know that liver veins draining directly into the atrium are located very anterior in the diaüphragm and therefore it is of utmost importance that liver venous outflow and right atrium need to mobilize extensively with a bid opening in the diaphragm to guarantee optimal venous outflow.
In conclusion, liver transplantation with partial or whole grafts is technically challenging in vascular abnormalities.
[1] Situs inversus
[2] dextrocardia
[3] cava aplasia
