
Pattern of CYP3A5 and MDR-1 single nucleotide polymorphism and its impact on tacrolimus levels and clinical outcomes in living renal allograft recipient
Raj Kanwar Yadav1, Sukhwinder Singh Sangha1, Asheesh Kumar1, V Seenu1, Sanjay K Agarwal1, Dipankar Bhowmik1.
1Dept of Nephrology, All India Institute of Medical Sciences, New Delhi, India
Introduction: Kidney transplant is best form of therapy for patients with end stage renal disease. Most favored immunosuppression in kidney transplant patients includes Tacrolimus, mycophenolate mofetil and steroids. Tacrolimus has narrow therapeutic index and requires therapeutic drug monitoring (TDM). However, there is wide variation in tacrolimus level with weight based fixed dosage regimens. This variability is due to polymorphism of major pathways of metabolism ie CYP3A5 and MDR1 genes. Fast metabolizer may require higher dosage and slow metabolizer may require lower dosage. Genotype based dosage strategy may be useful to achieve early therapeutic level and reduce episodes of rejections and major infections related. Methodology: 160 live related renal transplant patients at tertiary care hospital in India were included in this study from 2016 to 2018. Genetic polymorphism analysis in CYP3A5 and MDR1 gene was carried out at time of transplant. All patients were given a fixed weight-based dosage of Tacrolimus. Data was collected and analyzed in form of Tac levels, time to therapeutic levels, major infections and rejections in relation to genotype polymorphism.
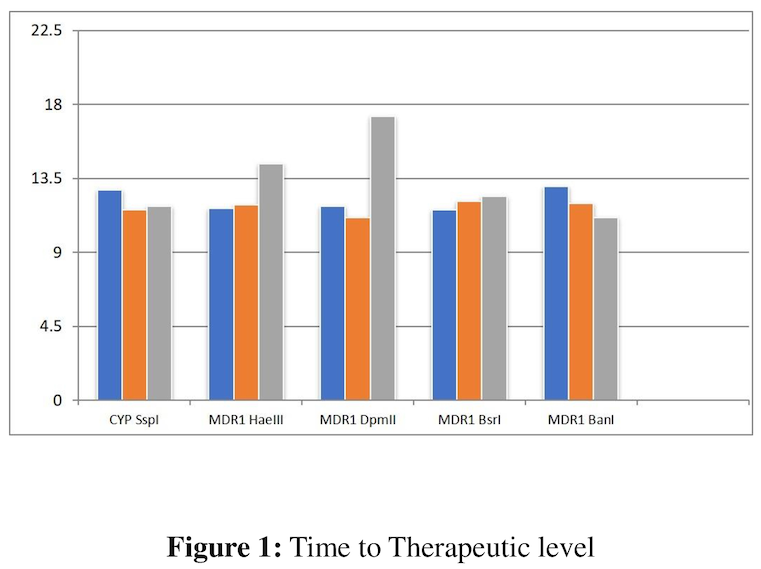
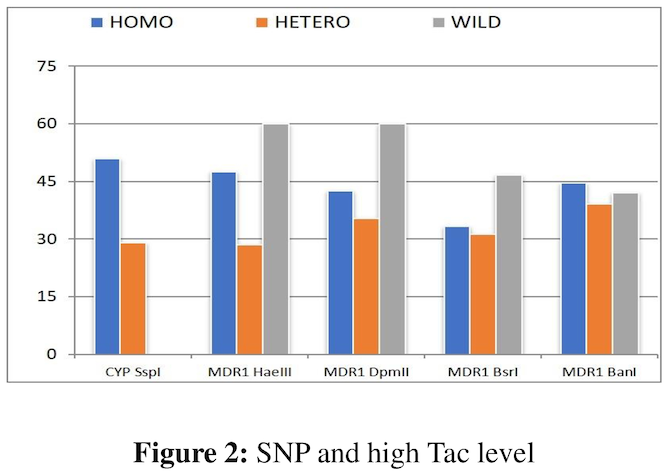
Results and discussion: 69.2% of Wild variants of CYP 3A5 (Expressors/Fast metabolizers) have initial low tac levels as compared to Homo variants (Non expressors/Slow metabolizers), 51.5% of whom have initial high tac levels. However, all variants achieve optimum tacrolimus levels at same time (mean 12.4 days). There were higher number of infections among homovariants attributable to initial high tacrolimus level. There were few numbers of rejections (8) which were not different among variants across genotypes.
Conclusion: Genotype based dosages can avoid initial high and low tac levels and possibly reduce number of infections among homovariants by avoiding initial high tacrolimus level. However, whether it will reduce episodes of rejections was not established in this study because of fewer number of rejection episodes.
[1] Tacrolimus level
[2] Gene Polymorphism
[3] Graft Rejection
[4] Immunosuppression
[5] Fast Metablolizers
