
A comparative study of early versus late initiation of renal replacement therapy in acute kidney injury due to snake envenomation and its impact on short-term and long-term outcome of the kidney function
Kaushik Mondal1, Pinaki Mukherjee1, Abhishek Mukherjee1, Tanima Bhattacharya1, Avishek Maity1.
1Nephrology, Nil Ratan Sircar Medical College, Kolkata, India
Introduction: Being one of the commonest causes of acute kidney injury (AKI) in India with variable outcomes, comprising of death, complete or partial or non-recovery, snake bite deserves utmost importance for timely intervention. Despite of high numbers of snake bite victims in India, there are no prospective studies regarding the timing of initiation of renal replacement therapy in such patients and its impact on the short-term and long-term changes in kidney function.
Methodology:
INCLUSION CRITERIA a. A definite history of snake bite. b. Clinical picture consistent with that of a hematotoxic snake bite. c. Age 18-65 years. d. Stage 2 acute kidney injury according to KDIGO classification. e. Informed consent provided by the patient or relatives.
EXCLUSION CRITERIA a. Patients presenting with stage 3 AKI as per KDIGO classification. b. Patients with evidence of pre-existing renal disease. c. Need for emergency renal replacement therapy even before randomization (Hyperkalemia > 6.5 mmol/l or metabolic acidosis with pH < 7.15 or volume overload refractory to diuretics with pulmonary edema). d. Patient received renal replacement therapy in outside hospital.
1. Early renal replacement therapy initiation strategy: Renal replacement therapy initiated within 12 hours of documentation of KDIGO stage 2 of acute kidney injury.
2. Delayed renal replacement initiation strategy: Patients in the delayed strategy group were initiated on dialysis 48 hours after documentation of KDIGO stage 2 of acute kidney injury.
Dialysis was not initiated in the delayed strategy group if spontaneous recovery of renal function occurred within the 48-hr observation period. Patients belonging to this group were monitored to detect the development of any one of the criteria for emergency dialysis. If needed, dialysis was initiated as soon as possible.
53 patients who fulfilled the inclusion criteria were randomized in 1:1 fashion to receive either early or delayed initiation of renal replacement therapy with written consent.Hemodialysis was continued till the patient became non-oliguric (urine output>500 ml/day) or there was decline of serum creatinine value to less than 1.5 mg/dl.
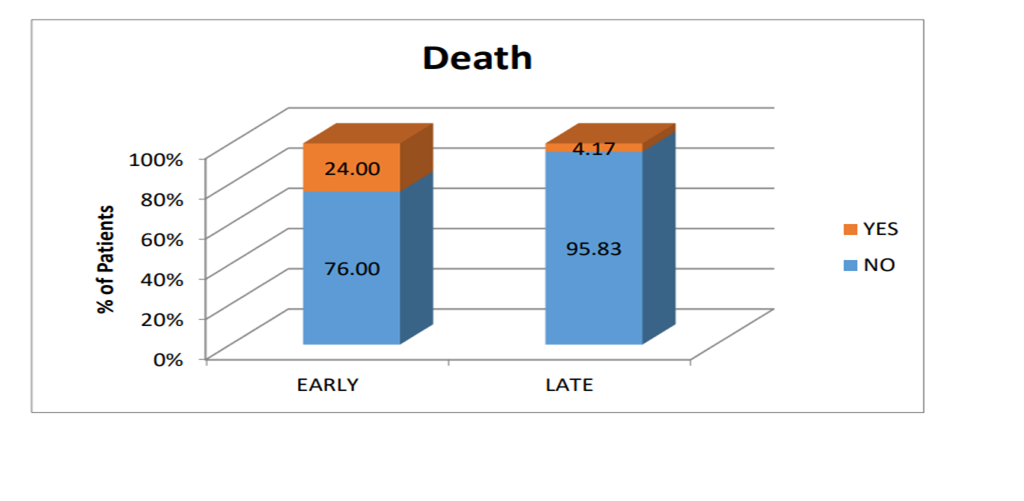
Results: Out of 25 patients of early initiative group, all had received Hemodialysis with 24% mortality and out of 28 patients of delayed initiative group, 86% received RRT with 4% mortality (p 0.047).
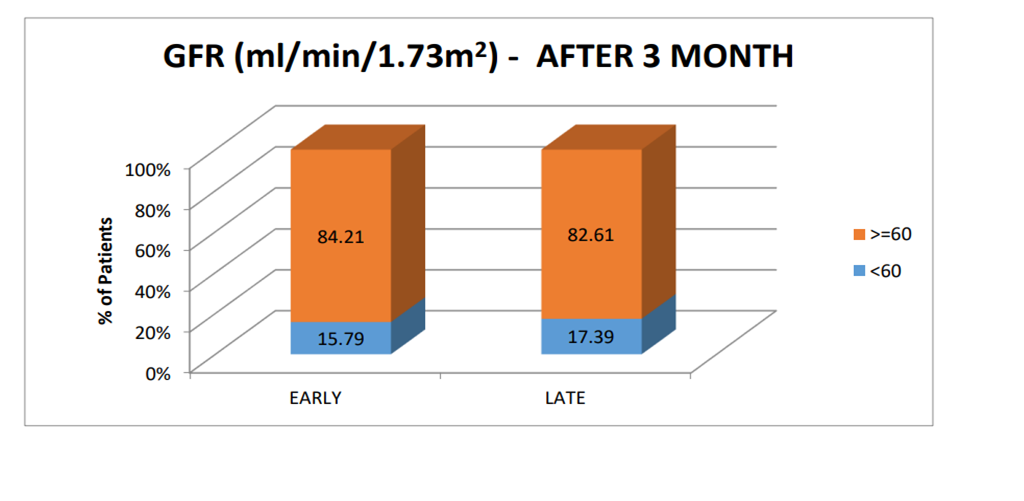
15% patients in the early renal replacement therapy initiation group and 17% patients in the delayed strategy group progressed to chronic kidney disease (p=0.890).
Mean proteinuria in patients given early RRT was 116.89 mg/day and in patients given late RRT was 143.57 mg/day after 90 days follow up (p=0.531).
Conclusions: There was increased mortality in patients assigned to the early initiation strategy of RRT compared to delayed initiation strategy with no significant difference in terms of progression from AKI to chronic kidney disease at the end of 90 days in the two groups of patients in snake-bite induced AKI.
